







You could prepare application for health care coverage pa 600 ch sg instantly in our PDFinity® online PDF tool. Our team is devoted to giving you the ideal experience with our editor by regularly adding new functions and upgrades. With these updates, using our editor becomes better than ever! By taking some basic steps, it is possible to begin your PDF journey:
Step 1: Access the PDF inside our editor by hitting the "Get Form Button" in the top section of this webpage.
Step 2: With our advanced PDF file editor, you'll be able to accomplish more than merely complete blanks. Try all of the features and make your docs appear sublime with custom textual content put in, or tweak the file's original input to excellence - all accompanied by the capability to incorporate any graphics and sign the PDF off.
Filling out this form calls for attentiveness. Ensure all required blank fields are done properly.
1. It's vital to complete the application for health care coverage pa 600 ch sg properly, so be attentive when working with the segments comprising all these fields:
2. Just after this section is filled out, go to type in the applicable details in all these - e v o m e R, n o, p m o c, r e, Last name ParentCaretaker, First Name, Middle Initial, Social Security Number, Street Address, City, County, State, Zip, Home Phone, and Work Phone.
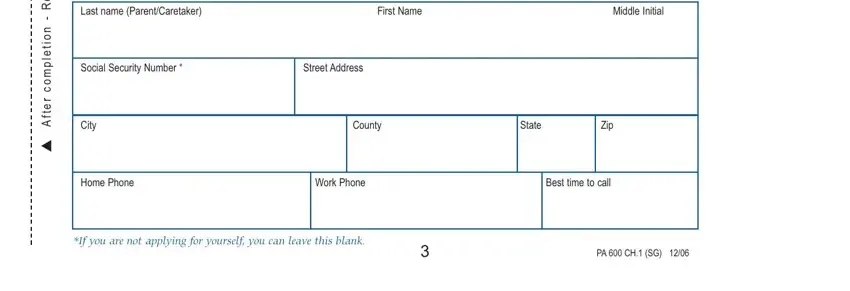
When it comes to e v o m e R and Street Address, be sure that you do everything properly in this current part. Both these are the most significant fields in the file.
3. Throughout this step, examine Last name first name MI, Yourself, Person, Person, Person, Person, Person, Are you applying for this person, Sex M or F, Is this person, Birthdate MMDDYY, Social Security Number, Is this person a student under age, How is this person related to you, and Is this person a US Citizen YesNo. Every one of these will need to be completed with greatest accuracy.
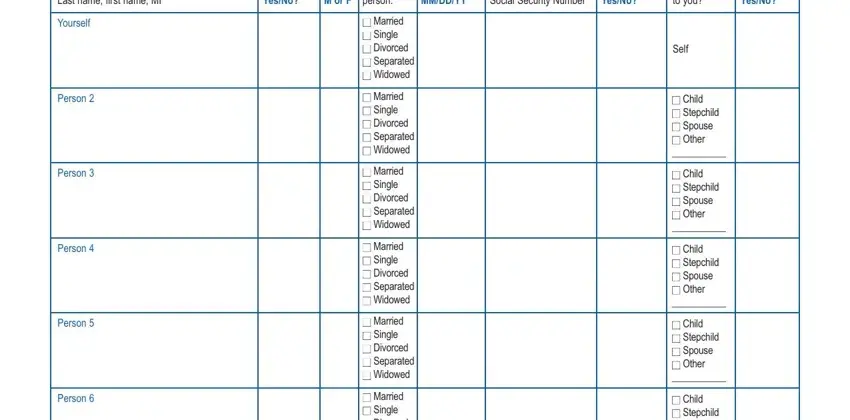
4. It is time to complete this next section! In this case you'll get all of these Person, Person, Married Single Divorced, Married Single Divorced, Married Single Divorced, Child Stepchild Spouse, Child Stepchild Spouse, Child Stepchild Spouse, If you are not applying for this, Are you or is anyone who lives, if the answer is no skip to, Do the stepchildren live with you, yes no, If yes tell us, and Stepparents name empty form fields to do.
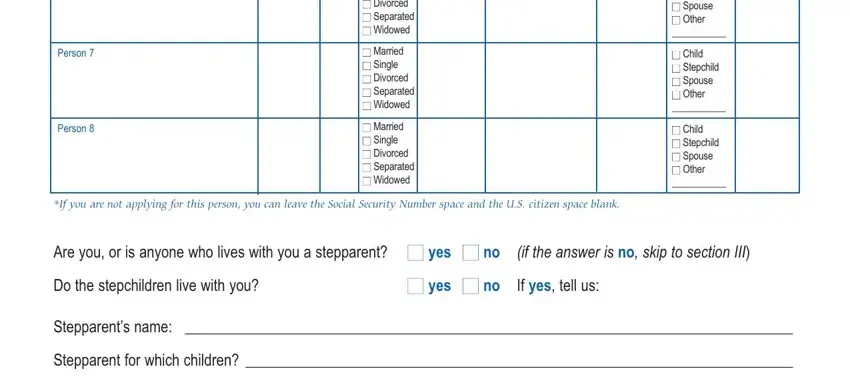
5. Lastly, the following last subsection is precisely what you'll want to finish before submitting the PDF. The blank fields here include the following: Stepparents name, Stepparent for which children, and PA CH SG.

Step 3: After rereading your completed blanks, press "Done" and you are good to go! Go for a 7-day free trial account with us and acquire instant access to application for health care coverage pa 600 ch sg - readily available in your FormsPal account. When you work with FormsPal, you can complete forms without worrying about data incidents or records getting distributed. Our secure software helps to ensure that your personal data is kept safely.