

Should you desire to fill out MMV, you won't need to download and install any kind of programs - just use our online PDF editor. To make our editor better and more convenient to utilize, we consistently develop new features, with our users' suggestions in mind. With a few basic steps, you can begin your PDF editing:
Step 1: Access the PDF form inside our tool by clicking the "Get Form Button" above on this page.
Step 2: The tool will give you the ability to customize your PDF document in a variety of ways. Modify it by adding customized text, adjust what is already in the document, and place in a signature - all within the reach of a couple of mouse clicks!
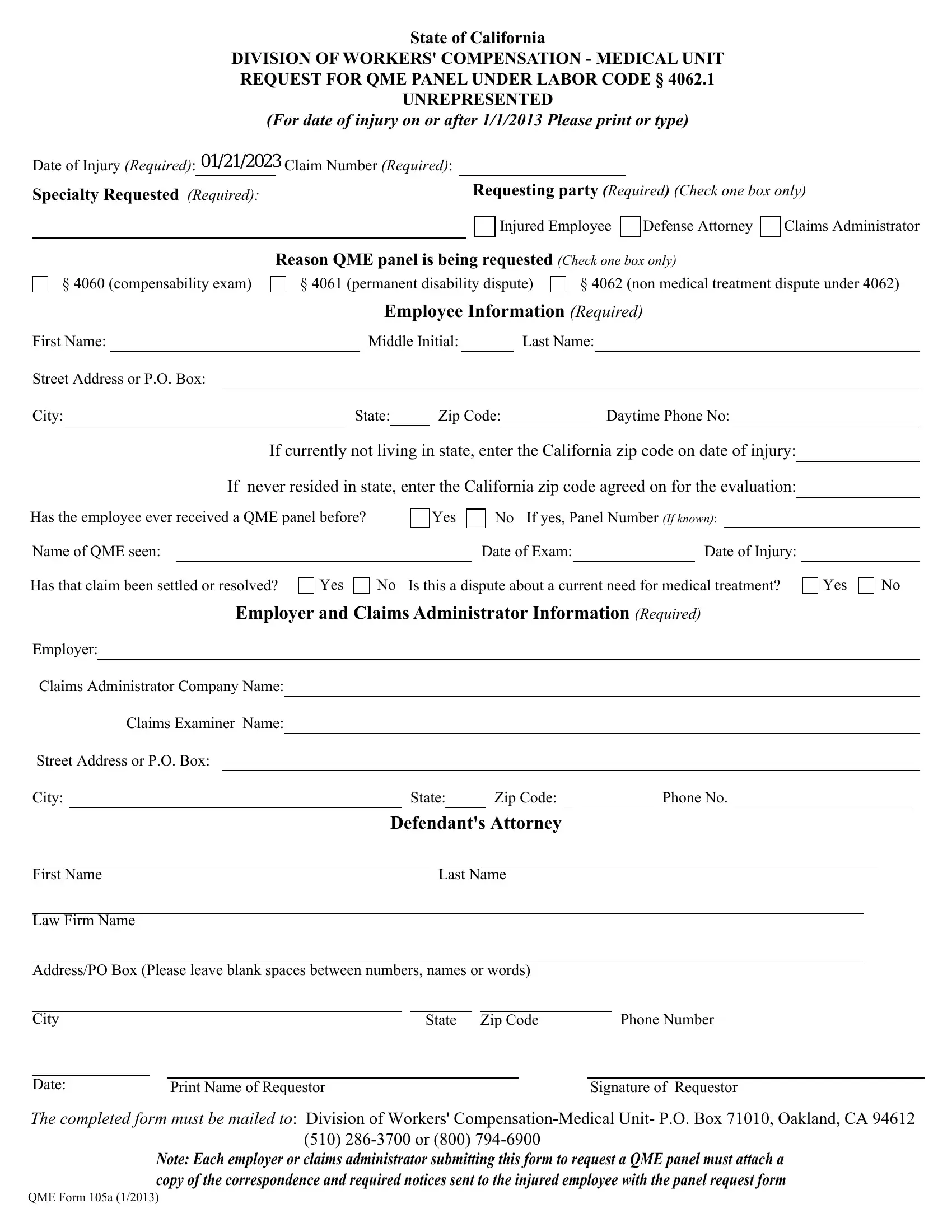
As a way to fill out this document, make sure that you provide the information you need in each and every blank field:
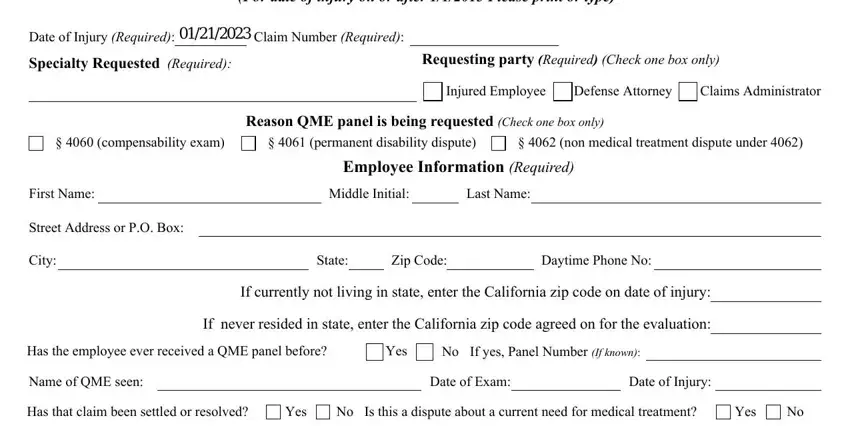
1. It's important to fill out the MMV properly, thus be attentive when filling in the areas comprising these blank fields:
2. Your next stage would be to fill in these particular fields: Employer and Claims Administrator, Employer, Claims Administrator Company Name, Claims Examiner Name, Street Address or PO Box, City, State, Zip Code, Phone No, First Name, Law Firm Name, Defendants Attorney, Last Name, AddressPO Box Please leave blank, and City.
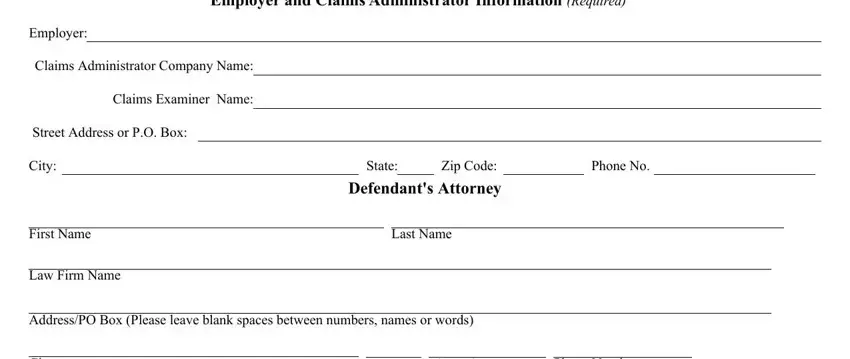
It's very easy to get it wrong while filling in the Last Name, thus make sure to take a second look before you'll send it in.
3. In this specific part, examine Date, State, Zip Code, Print Name of Requestor, Signature of Requestor, The completed form must be mailed, Note Each employer or claims, and QME Form a. These need to be taken care of with utmost precision.
Step 3: Right after you have looked once more at the details in the fields, simply click "Done" to finalize your FormsPal process. Right after setting up afree trial account with us, you'll be able to download MMV or send it via email without delay. The PDF form will also be accessible in your personal cabinet with your modifications. FormsPal is focused on the confidentiality of our users; we ensure that all information put into our tool remains confidential.