Are you in the midst of filing your taxes? If so, you’ve likely come across theRs 6037 form. Applying for this specific IRS form can be confusing and time consuming, but it is also an essential step in preparing accurate tax filings. This blog post will provide an in-depth look at all that comes with acquiring and filing a Rs 6037 form. Here, we will cover the requirements for requesting this document, how to apply for it effectively, and what actions to take if something goes wrong during the process. Read on to get everything you need to know about completing the Rs 6037 form with ease!
| Question | Answer |
|---|---|
| Form Name | Rs 6037 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | New_York, postretirement, subdivisions, ABOUTYOUR |
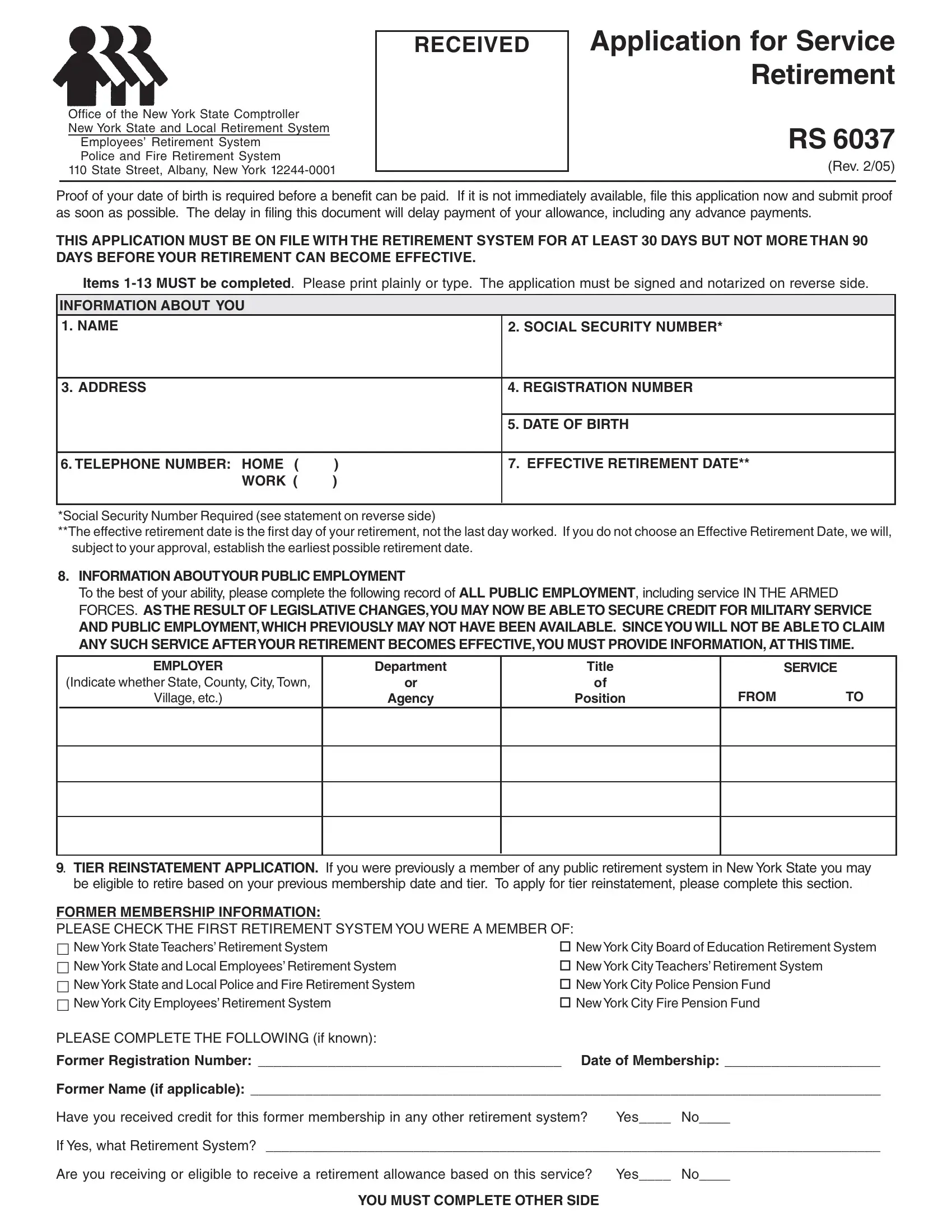
Office of the New York State Comptroller
New York State and Local Retirement System
Employees’ Retirement System
Police and Fire Retirement System
110 State Street, Albany, New York
RECEIVED
Application for Service Retirement
RS 6037
(Rev. 2/05)
Proof of your date of birth is required before a benefit can be paid. If it is not immediately available, file this application now and submit proof as soon as possible. The delay in filing this document will delay payment of your allowance, including any advance payments.
THIS APPLICATION MUST BE ON FILE WITH THE RETIREMENT SYSTEM FOR AT LEAST 30 DAYS BUT NOT MORE THAN 90 DAYS BEFORE YOUR RETIREMENT CAN BECOME EFFECTIVE.
Items
INFORMATION ABOUT YOU
1. NAME |
|
2. SOCIAL SECURITY NUMBER* |
|
|
|
3. ADDRESS |
|
4. REGISTRATION NUMBER |
|
|
|
|
|
5. DATE OF BIRTH |
|
|
|
6. TELEPHONE NUMBER: HOME ( |
) |
7. EFFECTIVE RETIREMENT DATE** |
WORK ( |
) |
|
|
|
|
*Social Security Number Required (see statement on reverse side)
**The effective retirement date is the first day of your retirement, not the last day worked. If you do not choose an Effective Retirement Date, we will, subject to your approval, establish the earliest possible retirement date.
8.INFORMATION ABOUTYOUR PUBLIC EMPLOYMENT
To the best of your ability, please complete the following record of ALL PUBLIC EMPLOYMENT, including service IN THE ARMED FORCES. AS THE RESULT OF LEGISLATIVE CHANGES,YOU MAY NOW BE ABLE TO SECURE CREDIT FOR MILITARY SERVICE
AND PUBLIC EMPLOYMENT, WHICH PREVIOUSLY MAY NOT HAVE BEEN AVAILABLE. SINCE YOU WILL NOT BE ABLE TO CLAIM ANY SUCH SERVICE AFTERYOUR RETIREMENT BECOMES EFFECTIVE,YOU MUST PROVIDE INFORMATION, AT THIS TIME.
EMPLOYER
(Indicate whether State, County, City, Town,
Village, etc.)
Department
or
Agency
Title
of
Position
SERVICE
FROMTO
9. TIER REINSTATEMENT APPLICATION. If you were previously a member of any public retirement system in New York State you may be eligible to retire based on your previous membership date and tier. To apply for tier reinstatement, please complete this section.
FORMER MEMBERSHIP INFORMATION:
PLEASE CHECK THE FIRST RETIREMENT SYSTEM YOU WERE A MEMBER OF:
New York State Teachers’ Retirement System |
New York City Board of Education Retirement System |
New York State and Local Employees’ Retirement System |
New York City Teachers’ Retirement System |
New York State and Local Police and Fire Retirement System |
New York City Police Pension Fund |
New York City Employees’ Retirement System |
New York City Fire Pension Fund |
PLEASE COMPLETE THE FOLLOWING (if known):
Former Registration Number: _______________________________________ Date of Membership: ____________________
Former Name (if applicable): _________________________________________________________________________________
Have you received credit for this former membership in any other retirement system? Yes____ No____
If Yes, what Retirement System? _______________________________________________________________________________
Are you receiving or eligible to receive a retirement allowance based on this service? Yes____ No____
YOU MUST COMPLETE OTHER SIDE
10. OTHER PUBLIC RETIREMENT SYSTEM MEMBERSHIPS: |
|
Are you currently a member of another public retirement system in New York State? Yes |
No |
Are you receiving or are you about to begin receiving a retirement benefit from any retirement system on the basis of employment
with New York State or any public entity in the State? |
Yes |
No |
If Yes, what Retirement System ________________________________ |
Registration Number _______________________ |
|
11.BENEFICIARY/OPTION INFORMATION FOR ESTIMATE. This is not the document on which you designate a beneficiary under your retirement option. You are required to make your option selection, and to designate your option beneficiary on a separate form, called a “Retirement Option Election Form.” If you have not filed a Retirement Option Election Form, we will be sending you one to complete and return. We are asking for the following information about your intended beneficiary for informational purposes. It will ensure that the estimate, upon which you make your option selection, is based on the correct beneficiary. Please look for the option election form in the mail and make sure you complete it and return it to us by the date we will request. We are not permitted by law to accept untimely option election forms. If your form is not timely filed, the Law requires an option which does not provide benefits to any beneficiary.
Estimate Beneficiary Information:
Beneficiary Name |
Date of Birth Gender (M/F) Spouse (Y/N) |
Item numbers 12 and 13 MUST be completed or your application will not be accepted.
12.PLEASE SIGN YOUR NAME IN FULL BELOW. Women should sign their own names, e.g. Jane Smith, NOT Mrs. John Smith.
I hereby make application for Service Retirement. I understand that this application may not be withdrawn on or after the effective date of my retirement.
________________________________________________
Signature (Sign Name in Full)
13. THIS ACKNOWLEDGEMENT MUST BE COMPLETED BYANOTARYPUBLIC.
State of ________________________________________ County of __________________________________
On the________ day of ____________ in the year __________ before me, the undersigned, personally appeared
_________________________________________________________________, personally known to me or proved to me on
the basis of satisfactory evidence to be the individual(s) whose name(s) is (are) subscribed to the within instrument and acknowledged to me that he/she/they executed the same in his/her/their capacity(ies), and that by his/her/their signature(s) on the instrument, the individual(s), or the person upon behalf of which the individual(s) acted, executed the instrument.
_______________________________________________
NOTARY PUBLIC (Please sign and affix stamp)
POST RETIREMENT EMPLOYMENT
Your paid public employment must cease at the time of your retirement. There are laws governing employment after retirement, and if you plan to be employed by or contract with a public employer, it is important for you to know about them. Failure to comply with these laws could result in the suspension or diminishment of your retirement allowance or termination of your retirement and reinstatement in the Retirement System as a new member.
Public employment is employment by, or contract with, the State of New York, one of its political subdivisions (county, city, town, village, school district) or some other public agency, such as a public authority. Employment by any other public employer located outside of New York State, employment by the Federal Government, or private employment does not need any approval and will in no way affect the retirement allowance paid to you by this Retirement System. Any questions concerning this most important matter should be directed to the New York State and Local Retirement System. By signing this application I hereby elect coverage under section 212 of the Retirement and Social Security Law, which permits me to earn from post- retirement public service annual amounts which do not exceed the limit provided in such section, without a resulting suspension or reduction of my retirement allowance.
HEALTH INSURANCE INFORMATION
The Retirement System does not administer Health Insurance Benefits. Any questions regarding this issue should be directed to your last employer.
PERSONAL PRIVACY PROTECTION LAW
The Retirement System is required by law to maintain records to determine eligibility for and calculate benefits. Failure to provide information may interfere with timely payment of benefits. The System may be required to provide certain information to participating employers. The official responsible for record maintenance is the Director of Member Services, NYS and Local Retirement System, Albany, NY 12244; call
*SOCIAL SECURITY DISCLOSURE REQUIREMENT
In accordance with the Federal Privacy Act of 1974 you are hereby advised that disclosure of your Social Security account number is mandatory pursuant to Section 11, 34, 311 and 334 of the Retirement and Social Security Law. Your number will be used in identifying your retirement records and in the administration of the Retirement System.