

Handling PDF forms online is a piece of cake using our PDF editor. You can fill out sglv 8600 fillable here and use many other options we offer. To make our tool better and more convenient to work with, we consistently design new features, taking into consideration suggestions coming from our users. Starting is simple! All that you should do is follow these easy steps below:
Step 1: Click the "Get Form" button at the top of this page to get into our tool.
Step 2: This tool enables you to customize PDF files in various ways. Improve it by including customized text, adjust what's originally in the PDF, and put in a signature - all doable in no time!
Completing this document generally requires attention to detail. Ensure each and every field is completed accurately.
1. When filling out the sglv 8600 fillable, be certain to complete all important fields in the corresponding area. This will help expedite the process, enabling your information to be processed quickly and appropriately.
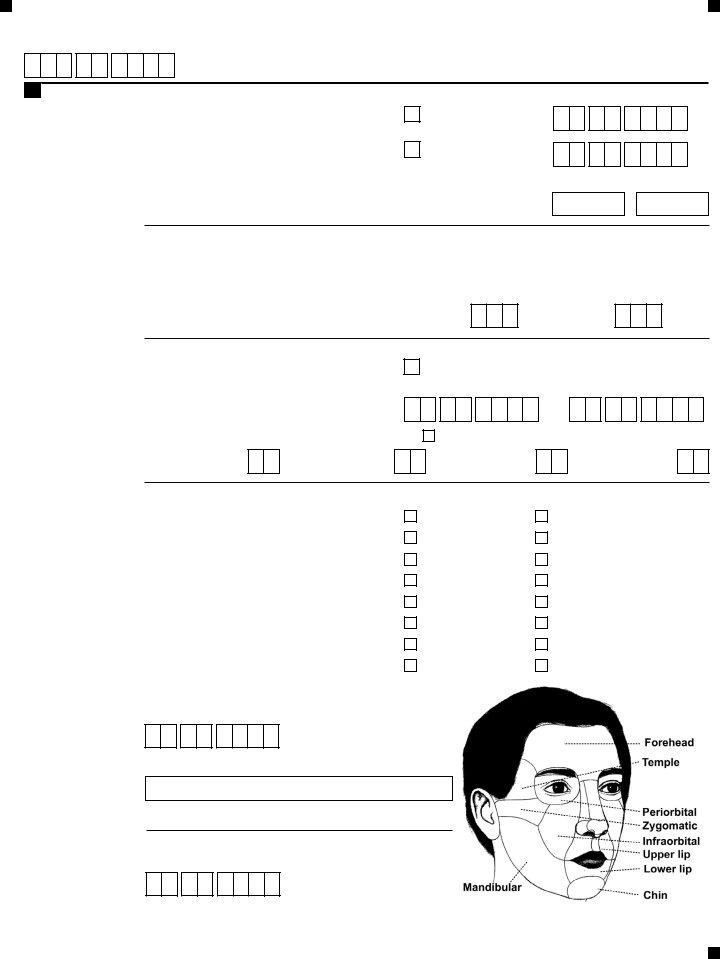
2. The subsequent step is to fill in these particular blanks: First Name, Guardian Power of Attorney or, Important Note Please include, Traumatic Injury Information, Last Name, Complete this section ONLY if a, Last Name, Mailing Address number and street, City, Telephone Number, Apartment if any, State, ZIP Code, Fax Number, and Injuries that Qualify for TSGLI.
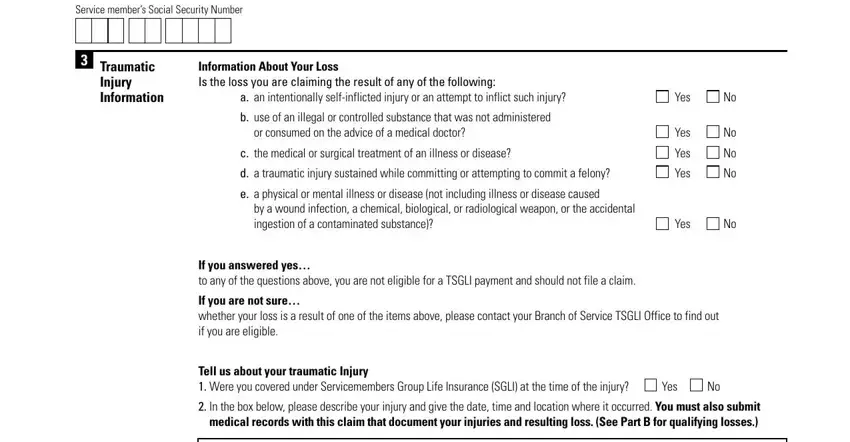
3. This 3rd segment is fairly easy, Service members Social Security, Traumatic Injury Information, Information About Your Loss Is the, a an intentionally selfinflicted, b use of an illegal or controlled, or consumed on the advice of a, c the medical or surgical, d a traumatic injury sustained, e a physical or mental illness or, Yes, Yes, Yes, Yes, by a wound infection a chemical, and Yes - these fields will have to be completed here.
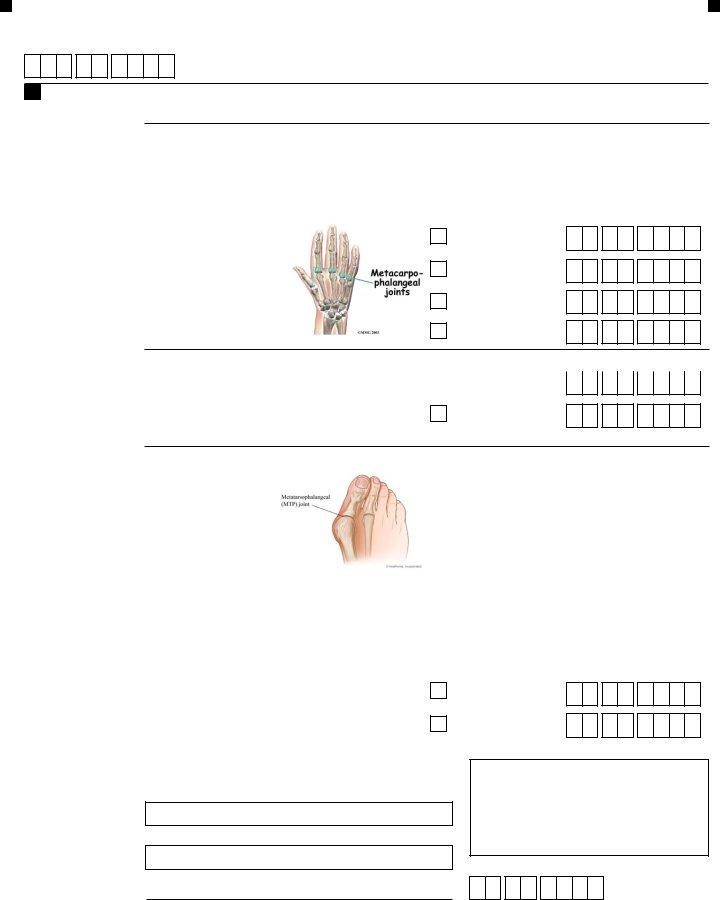
4. This fourth section comes next with these form blanks to fill out: Traumatic Injury Information.
5. The document needs to be wrapped up with this part. Below one can find an extensive list of form fields that have to be filled in with correct details to allow your document usage to be faultless: PART A Members Claim Information, Payment Options Please choose one, Payment Option Prudentials, Please choose one of the three, Payment Option Prudentials, Service members Mailing Address, Apartment Ward or Room if any, City, State, ZIP Code, Payment Option Electronic Funds, Bank Routing Number, Bank Account Number, Bank Name, and First Name.
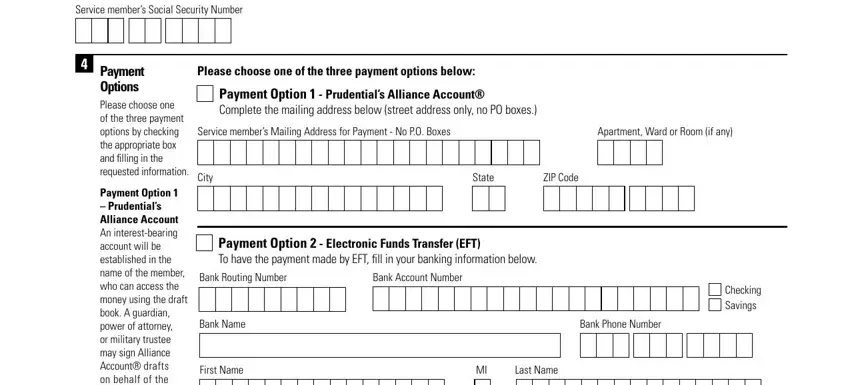
Be very careful when completing ZIP Code and Payment Option Prudentials, since this is the part in which most users make errors.
Step 3: Immediately after taking one more look at the fields and details, hit "Done" and you are all set! Sign up with us now and instantly gain access to sglv 8600 fillable, set for downloading. Every last edit you make is handily kept , making it possible to change the document at a later time if necessary. FormsPal is invested in the personal privacy of all our users; we make sure all information used in our tool continues to be secure.