
Handling PDF forms online is actually a piece of cake with our PDF tool. Anyone can fill out silver script pharmacy here and try out several other functions we offer. Our team is relentlessly working to expand the editor and ensure it is even easier for people with its many features. Bring your experience to the next level with constantly growing and exceptional opportunities available today! To get the process started, consider these easy steps:
Step 1: Firstly, open the tool by pressing the "Get Form Button" in the top section of this page.
Step 2: With our state-of-the-art PDF editor, you can actually accomplish more than merely fill out blank form fields. Try all of the features and make your forms seem sublime with customized text added, or fine-tune the original content to excellence - all that comes along with an ability to add your personal pictures and sign it off.
It's straightforward to finish the document using out detailed tutorial! This is what you must do:
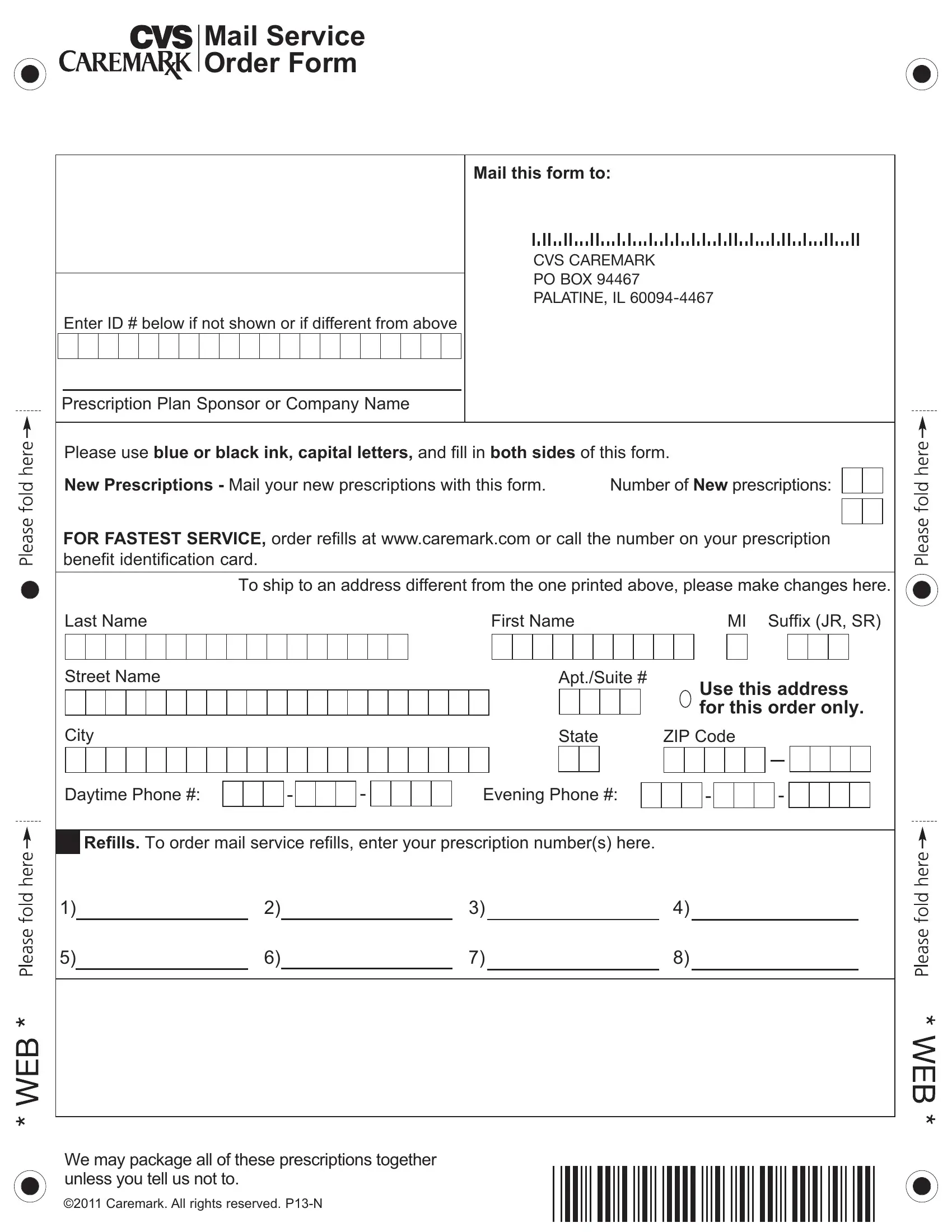
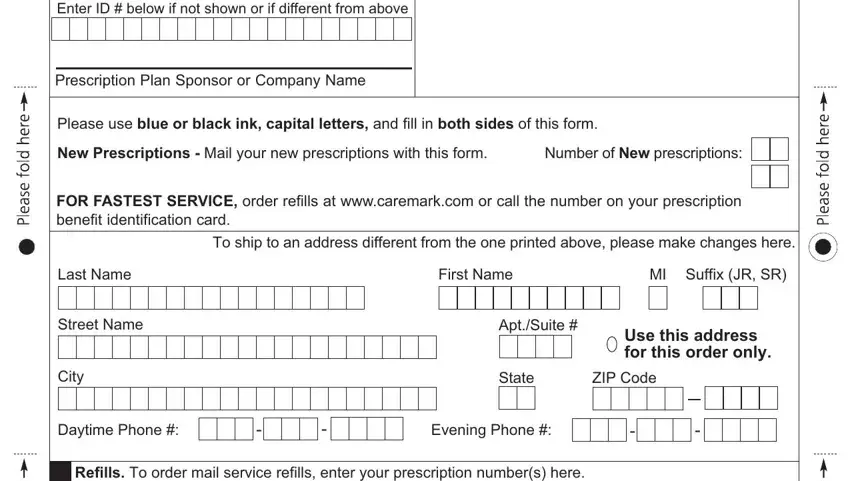
1. Fill out the silver script pharmacy with a group of major blanks. Gather all of the information you need and ensure nothing is forgotten!
2. Once the first part is filled out, go on to type in the relevant information in these: We may package all of these, and Caremark All rights reserved PN.
Be very mindful when filling in Caremark All rights reserved PN and Caremark All rights reserved PN, because this is the section in which many people make some mistakes.
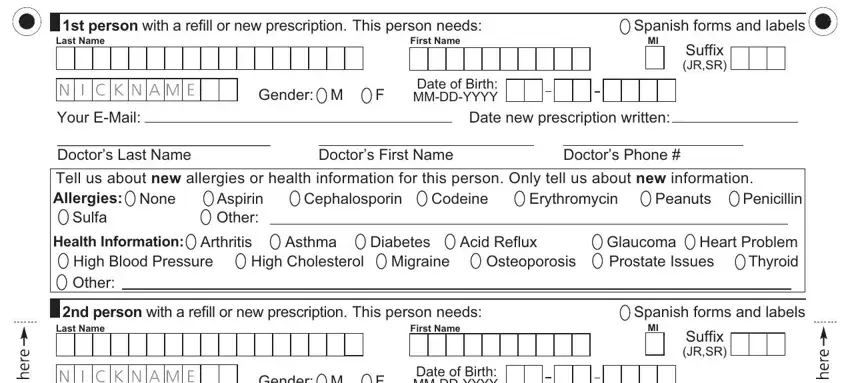
3. In this step, look at st person with a refill or new, First Name, Spanish forms and labels, Suffix JRSR, Your EMail, Date new prescription written, Gender M, Date of Birth MMDDYYYY, Doctors Last Name, Doctors First Name, Doctors Phone, Tell us about new allergies or, Cephalosporin, Erythromycin, and Codeine. All of these need to be filled out with highest focus on detail.
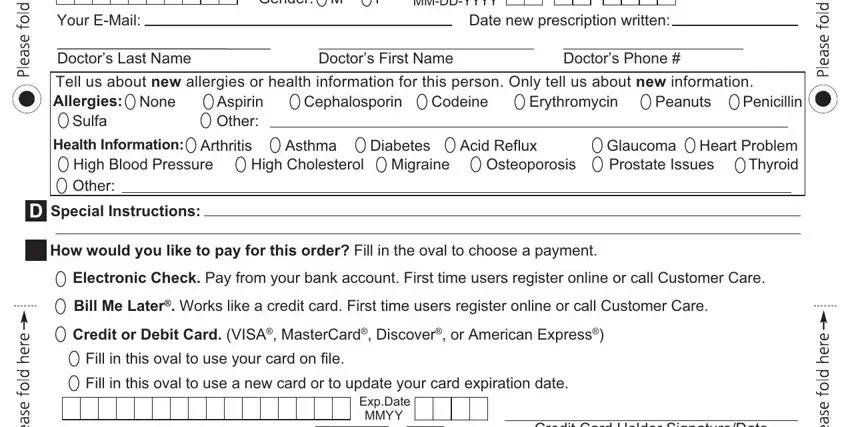
4. This next section requires some additional information. Ensure you complete all the necessary fields - Your EMail, Date new prescription written, Gender M, Date of Birth MMDDYYYY, Doctors Last Name, Doctors First Name, Doctors Phone, Tell us about new allergies or, Cephalosporin, Erythromycin, Peanuts, Codeine, Penicillin, Sulfa, and Aspirin Other - to proceed further in your process!
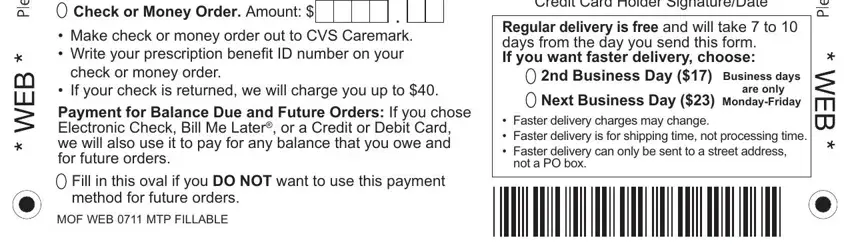
5. As you near the final parts of the file, there are a few more points to undertake. Mainly, Check or Money Order Amount, Make check or money order out to, Fill in this oval if you DO NOT, MOF WEB MTP FILLABLE, Credit Card Holder SignatureDate, Regular delivery is free and will, nd Business Day Business days, Next Business Day MondayFriday, are only, and Faster delivery charges may must all be done.
Step 3: You should make sure the information is right and click on "Done" to conclude the process. Right after setting up a7-day free trial account with us, it will be possible to download silver script pharmacy or email it right away. The PDF form will also be readily accessible in your personal account menu with your each and every modification. FormsPal offers safe form completion with no personal information record-keeping or sharing. Feel safe knowing that your data is safe here!