Are you looking for a way to easily and accurately submit information related to an individual’s disability benefits? Look no further than Standard Form 1411! This form is designed by the U.S. Department of Veterans Affairs (VA) as part of their Benefits Delivery System program and is required when applying for benefits related to service-connected disabilities such as VA health care, pension, education, Vocational Rehabilitation & Employment, insurance or burial. Read on to learn more about the purpose of Standard Form 1411 and its importance in accessing important services.
| Question | Answer |
|---|---|
| Form Name | Standart Form 1411 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | sf1411, standard form 1411 fillable, 1411, txr 1411 form |
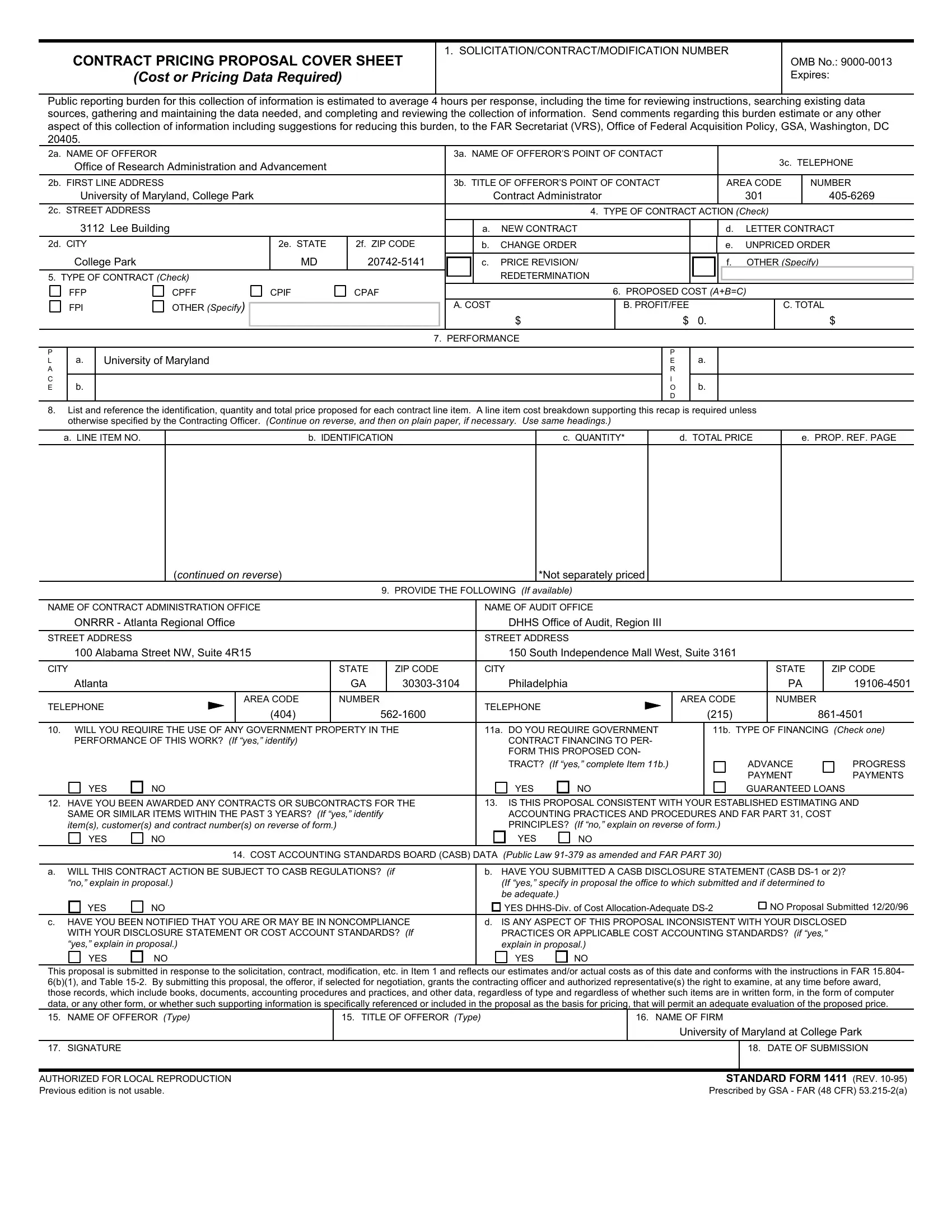
CONTRACT PRICING PROPOSAL COVER SHEET
(Cost or Pricing Data Required)
1. SOLICITATION/CONTRACT/MODIFICATION NUMBER
OMB No.:
Public reporting burden for this collection of information is estimated to average 4 hours per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information including suggestions for reducing this burden, to the FAR Secretariat (VRS), Office of Federal Acquisition Policy, GSA, Washington, DC 20405.
2a. NAME OF OFFEROR |
|
|
|
|
|
|
3a. NAME OF OFFEROR’S POINT OF CONTACT |
|
|
|
|
|
|
|
|
||||||
|
Office of Research Administration and Advancement |
|
|
|
|
|
|
|
|
|
|
|
|
3c. TELEPHONE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
2b. FIRST LINE ADDRESS |
|
|
|
|
|
|
3b. TITLE OF OFFEROR’S POINT OF CONTACT |
|
|
AREA CODE |
|
NUMBER |
|||||||||
|
University of Maryland, College Park |
|
|
|
|
|
|
Contract Administrator |
|
|
|
|
|
301 |
|
|
|
||||
2c. STREET ADDRESS |
|
|
|
|
|
|
|
|
4. TYPE OF CONTRACT ACTION (Check) |
|
|
|
|||||||||
|
3112 Lee Building |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
a. |
NEW CONTRACT |
|
|
|
|
d. |
LETTER CONTRACT |
||||||
2d. CITY |
|
|
|
2e. STATE |
2f. ZIP CODE |
|
|
|
b. |
CHANGE ORDER |
|
|
|
|
e. |
UNPRICED ORDER |
|||||
|
College Park |
|
|
MD |
|
|
|
c. |
PRICE REVISION/ |
|
|
|
|
f. |
OTHER (Specify) |
||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||
5. TYPE OF CONTRACT (Check) |
|
|
|
|
|
|
REDETERMINATION |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
FFP |
|
CPFF |
CPIF |
CPAF |
|
|
|
|
|
6. PROPOSED COST (A+B=C) |
|
|
|
|||||||
|
FPI |
|
OTHER (Specify) |
|
|
|
|
|
A. COST |
|
B. PROFIT/FEE |
|
|
|
|
|
C. TOTAL |
||||
|
|
|
|
|
|
|
|
|
|
|
$ |
$ |
0. |
|
|
|
|
$ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. PERFORMANCE |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P |
a. |
University of Maryland |
|
|
|
|
|
|
|
|
P |
a. |
|
|
|
|
|
|
|
||
L |
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|||||
A |
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
C |
b. |
|
|
|
|
|
|
|
|
|
|
|
I |
b. |
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
D |
|
|
|
|
|
|
|
|
8. |
List and reference the identification, quantity and total price proposed for each contract line item. A line item cost breakdown supporting this recap is required unless |
|
|
|
|||||||||||||||||
|
otherwise specified by the Contracting Officer. (Continue on reverse, and then on plain paper, if necessary. Use same headings.) |
|
|
|
|
|
|
|
|
|
|
||||||||||
a. LINE ITEM NO.
b. IDENTIFICATION
c. QUANTITY*
d. TOTAL PRICE
e. PROP. REF. PAGE
(continued on reverse)
*Not separately priced
9. PROVIDE THE FOLLOWING (If available)
NAME OF CONTRACT ADMINISTRATION OFFICE |
|
|
|
NAME OF AUDIT OFFICE |
|
|
|
|
|
|
|||||
ONRRR - Atlanta Regional Office |
|
|
|
|
DHHS Office of Audit, Region III |
|
|
|
|
|
|
||||
STREET ADDRESS |
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
|
|
|
100 Alabama Street NW, Suite 4R15 |
|
|
|
|
150 South Independence Mall West, Suite 3161 |
|
|
|
|
||||||
CITY |
|
|
|
STATE |
|
ZIP CODE |
CITY |
|
|
|
|
STATE |
|
ZIP CODE |
|
Atlanta |
|
|
|
GA |
|
|
Philadelphia |
|
|
|
|
PA |
|
||
TELEPHONE |
|
AREA CODE |
|
NUMBER |
|
|
TELEPHONE |
|
AREA CODE |
|
NUMBER |
|
|||
|
(404) |
|
|
|
(215) |
|
|||||||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
||||||||
10. WILL YOU REQUIRE THE USE OF ANY GOVERNMENT PROPERTY IN THE |
11a. |
DO YOU REQUIRE GOVERNMENT |
|
11b. TYPE OF FINANCING (Check one) |
|||||||||||
PERFORMANCE OF THIS WORK? (If “yes,” identify) |
|
|
|
|
CONTRACT FINANCING TO PER- |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
FORM THIS PROPOSED CON- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TRACT? (If “yes,” complete Item 11b.) |
|
|
ADVANCE |
PROGRESS |
|||
|
|
|
|
|
|
|
|
|
|
|
|
PAYMENT |
PAYMENTS |
||
YES |
NO |
|
|
|
|
YES |
NO |
|
|
GUARANTEED LOANS |
|||||
12. HAVE YOU BEEN AWARDED ANY CONTRACTS OR SUBCONTRACTS FOR THE |
13. |
IS THIS PROPOSAL CONSISTENT WITH YOUR ESTABLISHED ESTIMATING AND |
|||||||||||||
SAME OR SIMILAR ITEMS WITHIN THE PAST 3 YEARS? (If “yes,” identify |
|
ACCOUNTING PRACTICES AND PROCEDURES AND FAR PART 31, COST |
|
||||||||||||
item(s), customer(s) and contract number(s) on reverse of form.) |
|
|
|
|
PRINCIPLES? (If “no,” explain on reverse of form.) |
|
|
|
|
||||||
YES |
NO |
|
|
|
|
YES |
NO |
|
|
|
|
|
|
||
|
14. COST ACCOUNTING STANDARDS BOARD (CASB) DATA (Public Law |
|
|
|
|
||||||||||
|
|
||||||||||||||
a. WILL THIS CONTRACT ACTION BE SUBJECT TO CASB REGULATIONS? (if |
b. HAVE YOU SUBMITTED A CASB DISCLOSURE STATEMENT (CASB |
||||||||||||||
“no,” explain in proposal.) |
|
|
|
(If “yes,” specify in proposal the office to which submitted and if determined to |
|
||||||||||
|
|
|
|
|
|
|
be adequate.) |
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
|
YES |
|
NO Proposal Submitted 12/20/96 |
|||||||
c. HAVE YOU BEEN NOTIFIED THAT YOU ARE OR MAY BE IN NONCOMPLIANCE |
d. IS ANY ASPECT OF THIS PROPOSAL INCONSISTENT WITH YOUR DISCLOSED |
||||||||||||||
WITH YOUR DISCLOSURE STATEMENT OR COST ACCOUNT STANDARDS? (If |
PRACTICES OR APPLICABLE COST ACCOUNTING STANDARDS? (if “yes,” |
|
|||||||||||||
“yes,” explain in proposal.) |
|
|
|
explain in proposal.) |
|
|
|
|
|
|
|||||
YES |
NO |
|
|
|
|
YES |
NO |
|
|
|
|
|
|
||
This proposal is submitted in response to the solicitation, contract, modification, etc. in Item 1 and reflects our estimates and/or actual costs as of this date and conforms with the instructions in FAR 15.804- 6(b)(1), and Table
15. NAME OF OFFEROR (Type) |
15. TITLE OF OFFEROR (Type) |
16. NAME OF FIRM |
|
|
University of Maryland at College Park |
17. SIGNATURE
18. DATE OF SUBMISSION
AUTHORIZED FOR LOCAL REPRODUCTION |
STANDARD FORM 1411 (REV. |
Previous edition is not usable. |
Prescribed by GSA - FAR (48 CFR) |