Have you ever heard of State Form 28808? If not, it's important to know some of the basics to ensure that your business is compliant with governmental regulations. In this blog post, we'll discuss what State Form 28808 is, how businesses should use the form and why it's so important for staying on top of legal obligations and ensuring compliance. We'll also explore other aspects related to the form such as general filing rules and more specific information about when it needs to be used. By increasing your knowledge on this essential issue for any small or large business operation in your state, you can make sure that all your actions stay within the law.
| Question | Answer |
|---|---|
| Form Name | State Form 28808 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | state 28808 form, state form 28808 indiana 2017, state indiana 28808, dcs invoice form 28808 |
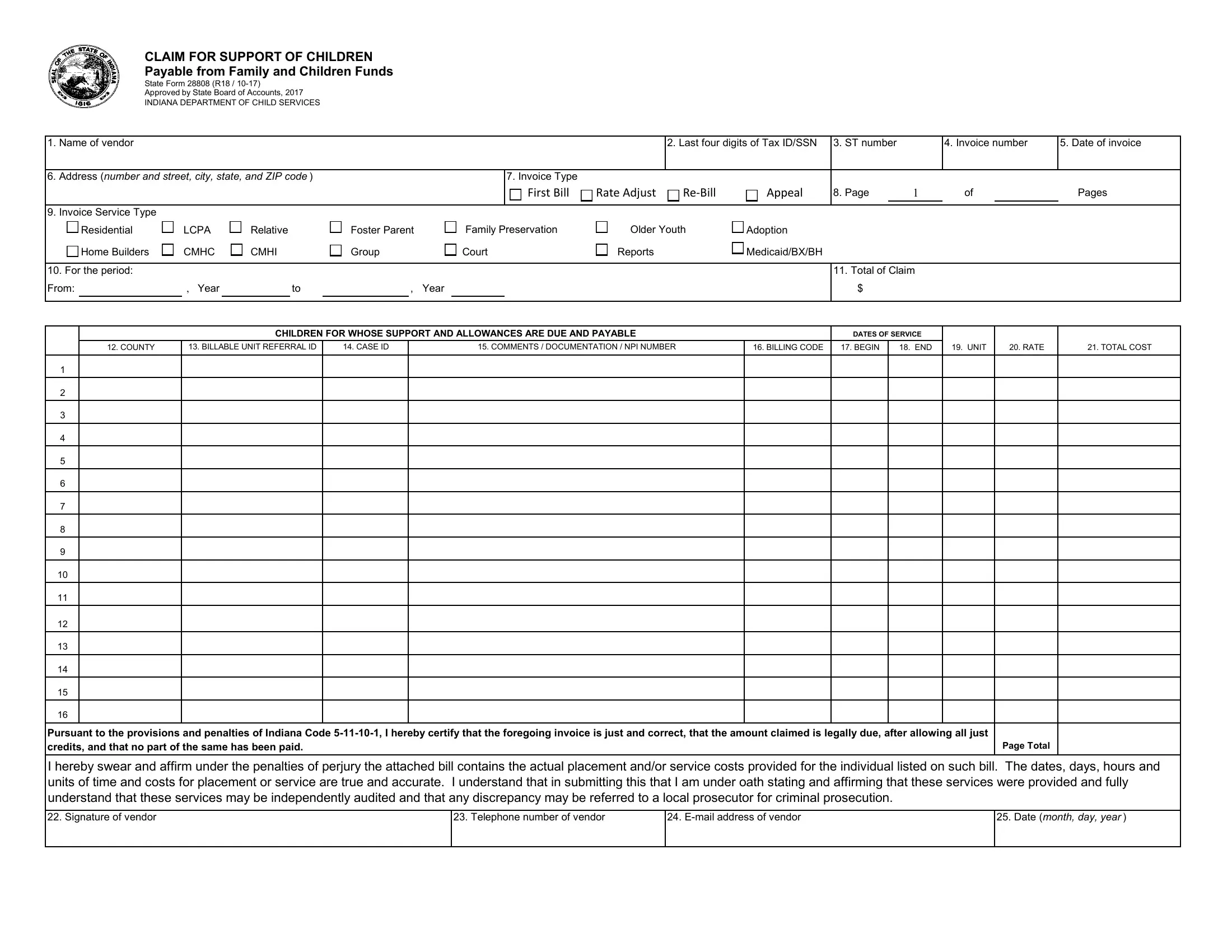
CLAIM FOR SUPPORT OF CHILDREN
Payable from Family and Children Funds
State Form 28808 (R18 /
Approved by State Board of Accounts, 2017
INDIANA DEPARTMENT OF CHILD SERVICES
1. |
Name of vendor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Last four digits of Tax ID/SSN |
3. ST number |
|
4. Invoice number |
5. Date of invoice |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6. |
Address (number and street, city, state, and ZIP code ) |
|
|
|
|
|
|
|
7. Invoice Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Bill |
|
|
Rate Adjust |
|
|
Appeal |
8. Page |
1 |
of |
|
Pages |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Invoice Service Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Residential |
|
|
LCPA |
|
|
|
Relative |
|
|
Foster Parent |
|
|
Family Preservation |
|
|
|
Older Youth |
|
|
Adoption |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
Home Builders |
|
|
CMHC |
|
|
|
CMHI |
|
|
Group |
|
|
Court |
|
|
|
Reports |
|
|
Medicaid/BX/BH |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. For the period: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Total of Claim |
|
|
|
|||||||
From: |
|
, Year |
|
|
|
|
to |
|
|
|
, Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
CHILDREN FOR WHOSE SUPPORT AND ALLOWANCES ARE DUE AND PAYABLE |
|
|
DATES OF SERVICE |
|
|
|
||||||||||||||||||||||
|
|
|
12. COUNTY |
13. BILLABLE UNIT REFERRAL ID |
|
|
14. CASE ID |
|
15. COMMENTS / DOCUMENTATION / NPI NUMBER |
16. BILLING CODE |
17. BEGIN |
18. END |
19. UNIT |
20. RATE |
21. TOTAL COST |
|||||||||||||||||||||||
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
7 |
|
8 |
|
9 |
|
10 |
|
11 |
|
12 |
|
13 |
|
14 |
|
15 |
|
16 |
|
Pursuant to the provisions and penalties of Indiana Code |
Page Total |
credits, and that no part of the same has been paid. |
I hereby swear and affirm under the penalties of perjury the attached bill contains the actual placement and/or service costs provided for the individual listed on such bill. The dates, days, hours and units of time and costs for placement or service are true and accurate. I understand that in submitting this that I am under oath stating and affirming that these services were provided and fully understand that these services may be independently audited and that any discrepancy may be referred to a local prosecutor for criminal prosecution.
22. Signature of vendor
23. Telephone number of vendor
24.
25.Date (month, day, year )
CLAIM FOR SUPPORT OF CHILDREN
Payable from Family and Children Funds
State Form 28808 (R18 /
Approved by State Board of Accounts, 2017
INDIANA DEPARTMENT OF CHILD SERVICES
1. |
Name of vendor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Last four digits of Tax ID/SSN |
3. ST number |
|
4. Invoice number |
5. Date of invoice |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6. |
Address (number and street, city, state, and ZIP code ) |
|
|
|
|
|
|
|
7. Invoice Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Bill |
|
|
Rate Adjust |
|
|
|
|
Appeal |
8. Page |
1 |
of |
|
Pages |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Invoice Service Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Residential |
|
|
LCPA |
|
|
|
Relative |
|
|
Foster Parent |
|
|
Family Preservation |
|
Older Youth |
|
|
Adoption |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
Home Builders |
|
|
CMHC |
|
|
|
CMHI |
|
|
Group |
|
|
Court |
|
Reports |
|
|
Medicaid/BX/BH |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. For the period: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Total of Claim |
|
|
|
|||||||
From: |
|
, Year |
|
|
|
|
to |
|
|
|
, Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
CHILDREN FOR WHOSE SUPPORT AND ALLOWANCES ARE DUE AND PAYABLE |
|
|
|
|
DATES OF SERVICE |
|
|
|
||||||||||||||||||||
|
|
|
12. COUNTY |
13. BILLABLE UNIT REFERRAL ID |
|
|
14. CASE ID |
|
15. COMMENTS / DOCUMENTATION / NPI NUMBER |
|
|
16. BILLING CODE |
17. BEGIN |
18. END |
19. UNIT |
20. RATE |
21. TOTAL COST |
|||||||||||||||||||||
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
7 |
|
8 |
|
9 |
|
10 |
|
11 |
|
12 |
|
13 |
|
14 |
|
15 |
|
16 |
|
Pursuant to the provisions and penalties of Indiana Code |
Page Total |
credits, and that no part of the same has been paid. |
I hereby swear and affirm under the penalties of perjury the attached bill contains the actual placement and/or service costs provided for the individual listed on such bill. The dates, days, hours and units of time and costs for placement or service are true and accurate. I understand that in submitting this that I am under oath stating and affirming that these services were provided and fully understand that these services may be independently audited and that any discrepancy may be referred to a local prosecutor for criminal prosecution.
22. Signature of vendor
23. Telephone number of vendor
24.
25.Date (month, day, year )
CLAIM FOR SUPPORT OF CHILDREN
Payable from Family and Children Funds
State Form 28808 (R18 /
Approved by State Board of Accounts, 2017
INDIANA DEPARTMENT OF CHILD SERVICES
1. |
Name of vendor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Last four digits of Tax ID/SSN |
3. ST number |
|
4. Invoice number |
5. Date of invoice |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
6. |
Address (number and street, city, state, and ZIP code ) |
|
|
|
|
|
|
|
7. Invoice Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Bill |
|
|
Rate Adjust |
|
|
|
|
Appeal |
8. Page |
1 |
of |
|
Pages |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Invoice Service Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Residential |
|
|
LCPA |
|
|
|
Relative |
|
|
Foster Parent |
|
|
Family Preservation |
|
Older Youth |
|
|
Adoption |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
Home Builders |
|
|
CMHC |
|
|
|
CMHI |
|
|
Group |
|
|
Court |
|
Reports |
|
|
Medicaid/BX/BH |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. For the period: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Total of Claim |
|
|
|
|||||||
From: |
|
, Year |
|
|
|
|
to |
|
|
|
, Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
CHILDREN FOR WHOSE SUPPORT AND ALLOWANCES ARE DUE AND PAYABLE |
|
|
|
|
DATES OF SERVICE |
|
|
|
||||||||||||||||||||
|
|
|
12. COUNTY |
13. BILLABLE UNIT REFERRAL ID |
|
|
14. CASE ID |
|
15. COMMENTS / DOCUMENTATION / NPI NUMBER |
|
|
16. BILLING CODE |
17. BEGIN |
18. END |
19. UNIT |
20. RATE |
21. TOTAL COST |
|||||||||||||||||||||
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
7 |
|
8 |
|
9 |
|
10 |
|
11 |
|
12 |
|
13 |
|
14 |
|
15 |
|
16 |
|
Pursuant to the provisions and penalties of Indiana Code |
Page Total |
credits, and that no part of the same has been paid. |
I hereby swear and affirm under the penalties of perjury the attached bill contains the actual placement and/or service costs provided for the individual listed on such bill. The dates, days, hours and units of time and costs for placement or service are true and accurate. I understand that in submitting this that I am under oath stating and affirming that these services were provided and fully understand that these services may be independently audited and that any discrepancy may be referred to a local prosecutor for criminal prosecution.
22. Signature of vendor
23. Telephone number of vendor
24.
25.Date (month, day, year )
INSTRUCTIONS FOR COMPLETING A CLAIM FOR SUPPORT OF CHILDREN
October 2017
*= Required field.
1.*NAME – Legal name of benefit/product/service provider; must match name submitted via the Vendor Information Form.
2.*LAST FOUR DIGITS OF TAX ID – The last four digits of the Federal Tax Identification Number associated with the legal name in Section 1. This is your Social Security Number for individuals (e.g.foster parents).
3.*ST NUMBER – State Vendor ID # assigned by the DCS payment system (KidTraks). This 6 digit number can be found on the Warrant Summary.
ST Numbers are also available at https://magik.dcs.in.gov/Portal/Home/Login?ReturnUrl=%2fportal%2f. From there, select "Provider Service Guide" and enter your Tax ID in the appropriate space provided.
4.*INVOICE NUMBER – assigned by the vendor; CAN BE NO LONGER THAN 8 CHARACTERS; should be a unique number for each submission and can include letters and/or numbers (e.g. "Nov2010" or "1001").
5.*DATE OF INVOICE – Date assigned by the vendor as the date of the claim. Invoices must be received by DCS KidTraks Invoicing within 10 business days of this date.
6.*ADDRESS – Vendor's complete address, which should match the most recent Vendor Information form on file.
7.*INVOICE TYPE – Is the invoice being submitted the first submission, a rate adjustment, a
8.*PAGE NUMBER – Includes the current page number as well as the total number of pages included in the Claim (limited to a total of 3 pages per Invoice).
9.*INVOICE SERVICE TYPE – Only one overriding service type should be picked for all sevice codes being invoice in column 16. The invoice service type should reflect all services being invoiced.
10.*FOR THE PERIOD – The beginning and end dates of the month being billed on the Claim. (e.g. January services would be: From January 1, 2011 to January 31, 2011).
The Claim period should not be confused with the Dates of Service (Sections 17 and 18) as vendors may list multiple children/Case #s/Referral IDs with different dates of service during the Claim period.
11.*TOTAL OF CLAIM – The cumulative sum of the Total Cost columns (col. 21) of all invoice pages
This total cannot be adjusted upward once it's been submitted.
12.*COUNTY – Name of County that authorized services to be rendered for the child being served. For Post Adoption or Independent Living services, please enter County of child’s residence. NOTE: An invoice can include line items for multiple counties.
13.*BILLABLE UNIT REFERRAL ID– Billable Unit Referral ID (PL# or RF#) for Service Referrals; Probation will still use Case number until fully implemented on the Referral Wizard.
14.*CASE ID – This is the case number in KidTraks and is required for all foster care invoices as well as all provider invoices for all services.
15.*COMMENTS / DOCUMENTATION / NPI NUMBER – Spaces can also be used to provide explanation / documentation to support payments and NPI number of doctor.
16.*BILLING CODE – Includes both Service and Component Codes for the benefit/product/service provided. Provider codes are available at https://magik.dcs.in.gov/Portal/Home/Login?ReturnUrl=%2fportal%2f From there, select "Provider Service Guide" and enter your Tax ID or DCS Vendor ID (i.e. ST Number) in the appropriate space provided.
17.*BEGIN DATE OF SERVICE – First day the benefit/product/service was provided. If the service was provided in one day, the Begin Date and End Dates will be the same.
18.*END OF DATE OF SERVICE – Last day the benefit/product/service was provided. If the service was provided in one day, the Begin Date and End Dates will be the same.
19.*UNIT – The number of times a benefit/product/service was rendered during the Claim period.
Units are defined in contracts/agreements and are typically
20.*RATE – The amount
21.*TOTAL COST – The total amount of the line item calculated by multiplying the number of units by the rate (Unit x Rate=Total Cost)
22.*SIGNATURE OF VENDOR – Authorizing signature of vendor submitting the Claim. All pages submitted must be signed; blue ink is strongly recommended.
23.* TELEPHONE NUMBER OF VENDOR – Telephone number for Vendor, to be used only for clarifications and resolution of billing issues.
24.
25.*DATE – This is the date the invoice was completed/signed. This date can not be before the last day of service.