Whether you’re a business owner, an accountant, or any other professional dealing with vehicle registration and titling fees in the state of Ohio, knowing when and how to file State Form 49937 is essential. This form can be extremely confusing if you don’t know what information needs to be included for each step of filing. To make sure that all necessary paperwork is filled out accurately and on time, it’s important to understand the basics behind State Form 49937. In this blog post we will break down exactly what document processing options are available with this form as well as answer some of the key questions around requirements for individual vehicles.
| Question | Answer |
|---|---|
| Form Name | State Form 49937 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Expiration, CERTIFICATION, CNA, ISDH |
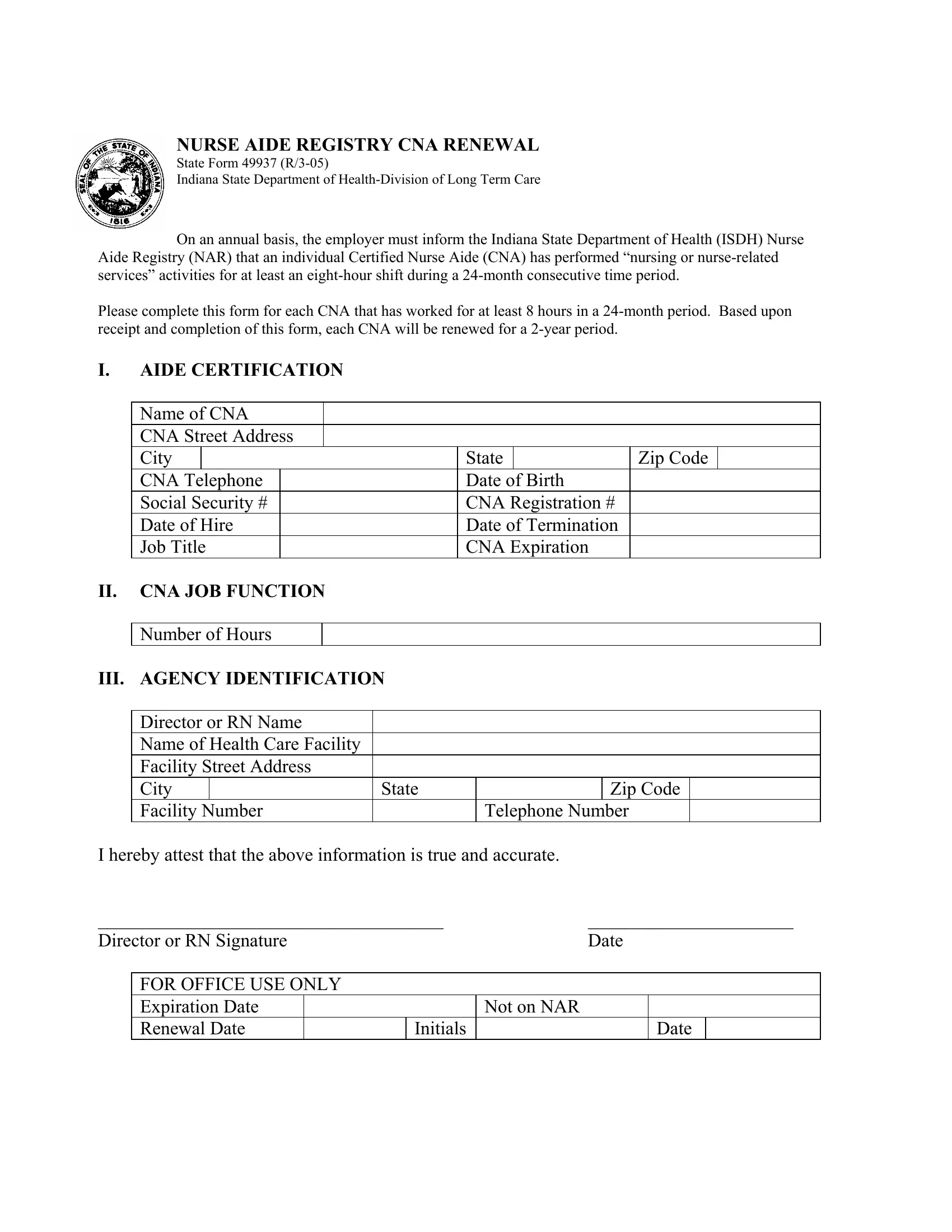
NURSE AIDE REGISTRY CNA RENEWAL
State Form 49937
Indiana State Department of
On an annual basis, the employer must inform the Indiana State Department of Health (ISDH) Nurse Aide Registry (NAR) that an individual Certified Nurse Aide (CNA) has performed “nursing or
Please complete this form for each CNA that has worked for at least 8 hours in a
I.AIDE CERTIFICATION
Name of CNA
CNA Street Address
City |
|
|
State |
|
Zip Code |
|
CNA Telephone |
|
Date of Birth |
|
|
||
Social Security # |
|
CNA Registration # |
|
|
||
Date of Hire |
|
Date of Termination |
|
|
||
Job Title |
|
CNA Expiration |
|
|
||
II.CNA JOB FUNCTION Number of Hours
III. AGENCY IDENTIFICATION
Director or RN Name |
|
|
Name of Health Care Facility |
|
|
Facility Street Address |
|
|
City |
State |
Zip Code |
Facility Number |
|
Telephone Number |
I hereby attest that the above information is true and accurate.
_____________________________________ |
______________________ |
|||||
Director or RN Signature |
|
Date |
||||
|
|
|
|
|
|
|
|
FOR OFFICE USE ONLY |
|
|
|
|
|
|
Expiration Date |
|
|
Not on NAR |
|
|
|
Renewal Date |
|
Initials |
|
Date |
|