
Handling PDF documents online is certainly very simple with this PDF editor. Anyone can fill in Form Std 692 here effortlessly. Our editor is constantly developing to give the very best user experience attainable, and that is thanks to our resolve for constant improvement and listening closely to feedback from customers. This is what you will want to do to start:
Step 1: Press the "Get Form" button in the top section of this page to access our editor.
Step 2: With this state-of-the-art PDF editor, you'll be able to do more than just fill in blank fields. Express yourself and make your docs appear perfect with customized textual content added in, or modify the file's original content to perfection - all comes with the capability to incorporate any type of images and sign it off.
Be mindful while completing this document. Ensure each and every blank is filled out accurately.
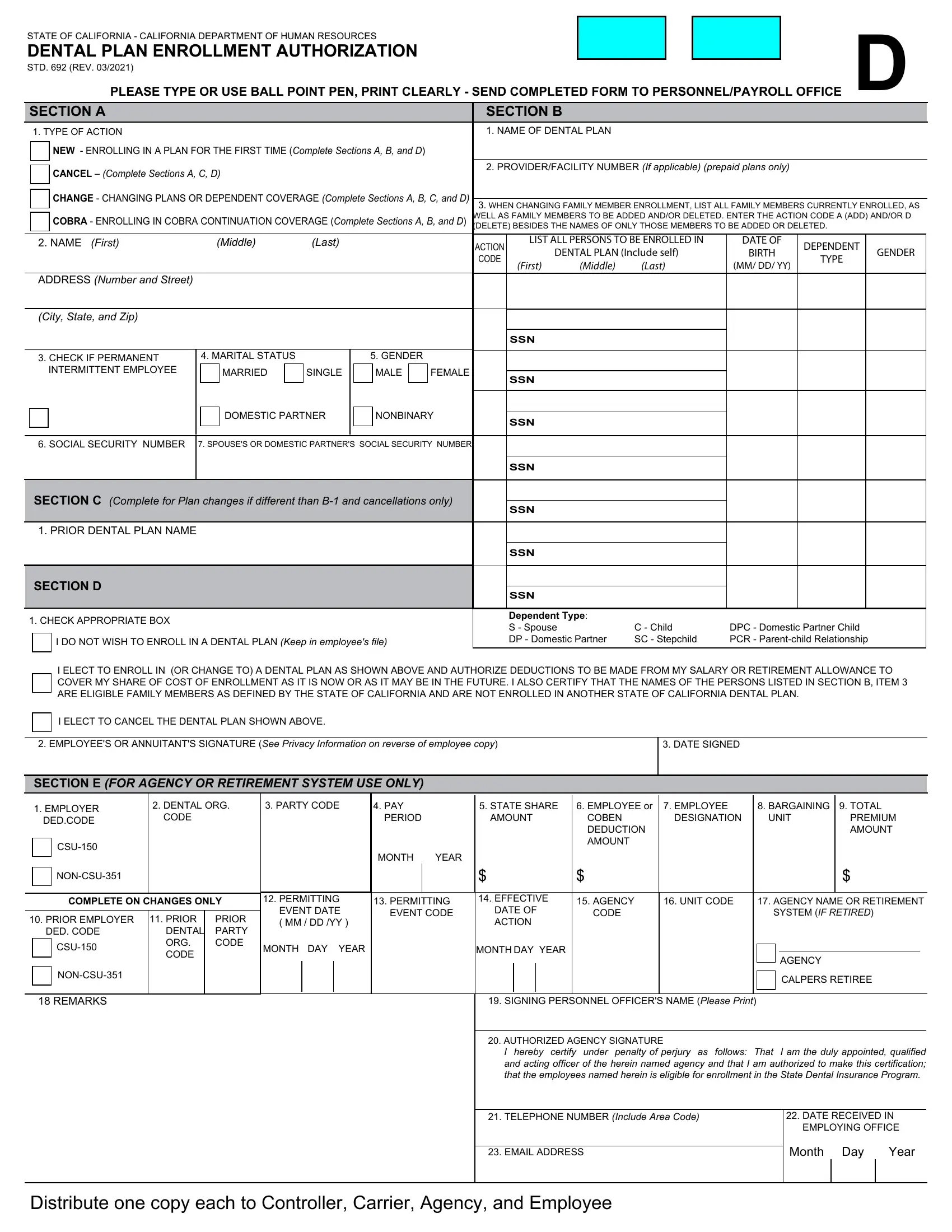
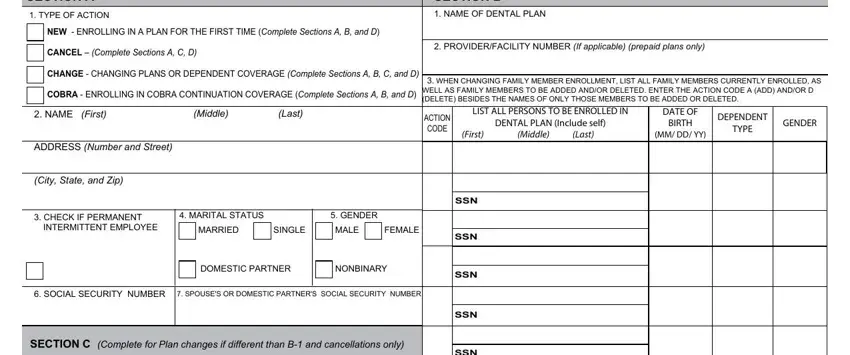
1. When filling in the Form Std 692, make certain to complete all important fields in its relevant section. It will help to speed up the process, which allows your information to be handled promptly and properly.
2. Right after the last array of blanks is filled out, go to enter the suitable information in these - PRIOR DENTAL PLAN NAME, SECTION D, CHECK APPROPRIATE BOX, I DO NOT WISH TO ENROLL IN A, SSN, SSN, SSN, Dependent Type S Spouse DP, C Child SC Stepchild, DPC Domestic Partner Child PCR, I ELECT TO ENROLL IN OR CHANGE TO, I ELECT TO CANCEL THE DENTAL PLAN, EMPLOYEES OR ANNUITANTS SIGNATURE, DATE SIGNED, and SECTION E FOR AGENCY OR RETIREMENT.
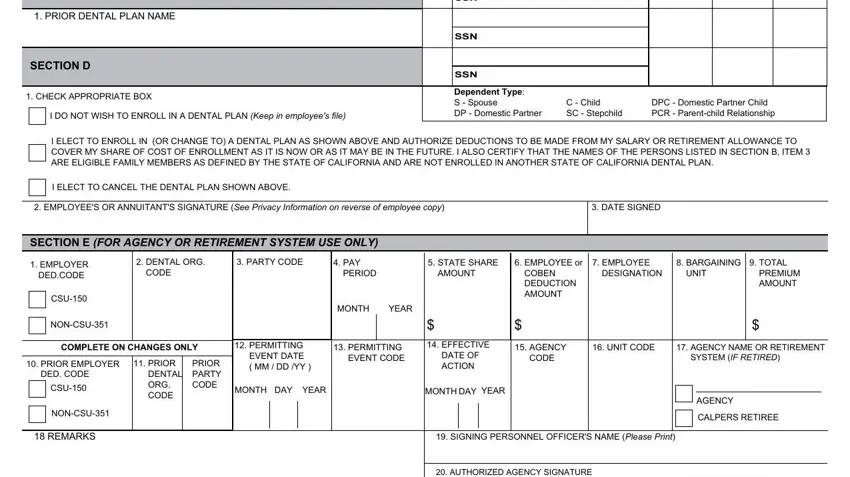
3. The next step is easy - fill in every one of the fields in I hereby certify under penalty of, TELEPHONE NUMBER Include Area Code, EMAIL ADDRESS, DATE RECEIVED IN EMPLOYING OFFICE, Month Day, Year, and Distribute one copy each to in order to finish the current step.

You can certainly make a mistake when filling out the Year, thus make sure to reread it prior to deciding to send it in.
Step 3: Prior to addressing the next step, it's a good idea to ensure that all blanks have been filled in the correct way. When you verify that it is good, press “Done." Obtain the Form Std 692 once you sign up for a free trial. Readily get access to the pdf form within your FormsPal account, with any modifications and adjustments all preserved! Here at FormsPal, we do our utmost to be certain that your details are stored private.