Are you a resident or potential patient living in an area serviced by Suburban Hospital? Then it's important to know about Form SB 2160. This form is used by the hospital to ensure that all patients receive their medical records swiftly, securely and confidentially. Whether you're new to the neighborhood or a longtime visitor at Suburban Hospital, understanding why and how this form works can help save time during your next visit and guarantee compliance with local health regulations. In this blog post, we'll explain exactly what Form SB 2160 is, why it's required for care at Suburban Hospital and how you can use it when scheduling appointments or filing appeals related to your healthcare conditions.
| Question | Answer |
|---|---|
| Form Name | Suburban Hospital Form Sb 2160 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Payors, BMI, CPAP, NPI |
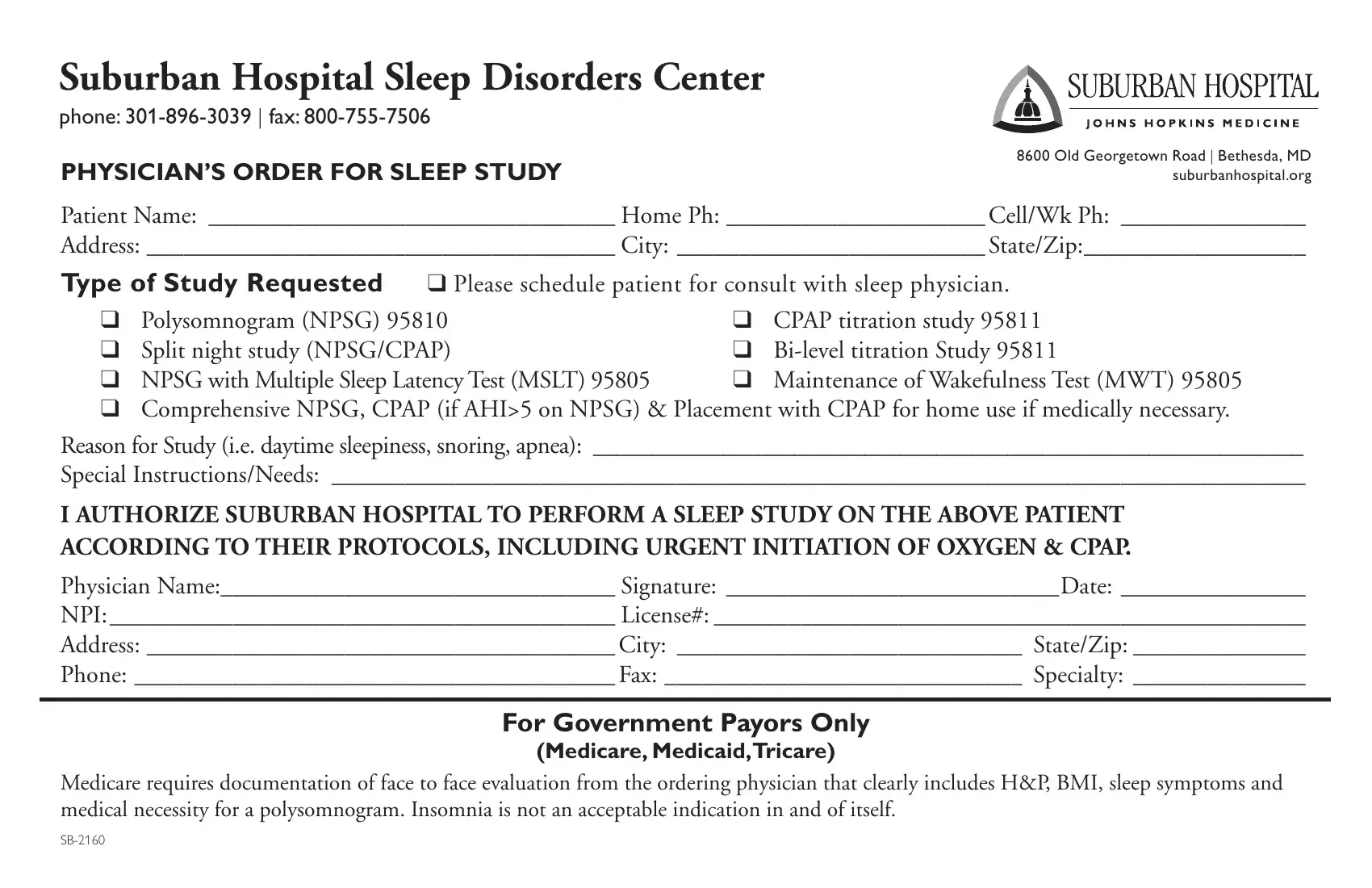
Suburban Hospital Sleep Disorders Center
phone:
PHYSICIAN’S ORDER FOR SLEEP STUDY
8600 Old Georgetown Road | Bethesda, MD suburbanhospital.org
Patient Name: _________________________________ Home Ph: _____________________ Cell/Wk Ph: _______________
Address: ______________________________________ City: _________________________ State/Zip:__________________
Type of Study Requested q Please schedule patient for consult with sleep physician.
q |
Polysomnogram (NPSG) 95810 |
q CPAP titration study 95811 |
|
q Split night study (NPSG/CPAP) |
q |
||
q |
NPSG with Multiple Sleep Latency Test (MSLT) 95805 |
q |
Maintenance of Wakefulness Test (MWT) 95805 |
qComprehensive NPSG, CPAP (if AHI>5 on NPSG) & Placement with CPAP for home use if medically necessary.
Reason for Study (i.e. daytime sleepiness, snoring, apnea): ____________________________________________________________
Special Instructions/Needs: _______________________________________________________________________________
I AUTHORIZE SUBURBAN HOSPITAL TO PERFORM A SLEEP STUDY ON THE ABOVE PATIENT ACCORDING TO THEIR PROTOCOLS, INCLUDING URGENT INITIATION OF OXYGEN & CPAP.
Physician Name:________________________________ Signature: ___________________________Date: _______________
NPI: _________________________________________ License#: ________________________________________________
Address: ______________________________________ City: ____________________________ State/Zip: ______________
Phone: _______________________________________ Fax: _____________________________ Specialty: ______________
For Government Payors Only
(Medicare, Medicaid,Tricare)
Medicare requires documentation of face to face evaluation from the ordering physician that clearly includes H&P, BMI, sleep symptoms and medical necessity for a polysomnogram. Insomnia is not an acceptable indication in and of itself.