Are you looking for a simple way to manage, store, and organize all your data? With the TR Form DB 4 software program, you can do just that — all in one convenient package. This powerful piece of software was designed with users in mind and provides an intuitive interface that makes managing your information easier than ever! Keep reading for more details on this innovative form management solution and discover how it can streamline your workflow today.
| Question | Answer |
|---|---|
| Form Name | Trs Form Db 4 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | physicians, Georgia, print disability forms texas, trs disability retirement texas |
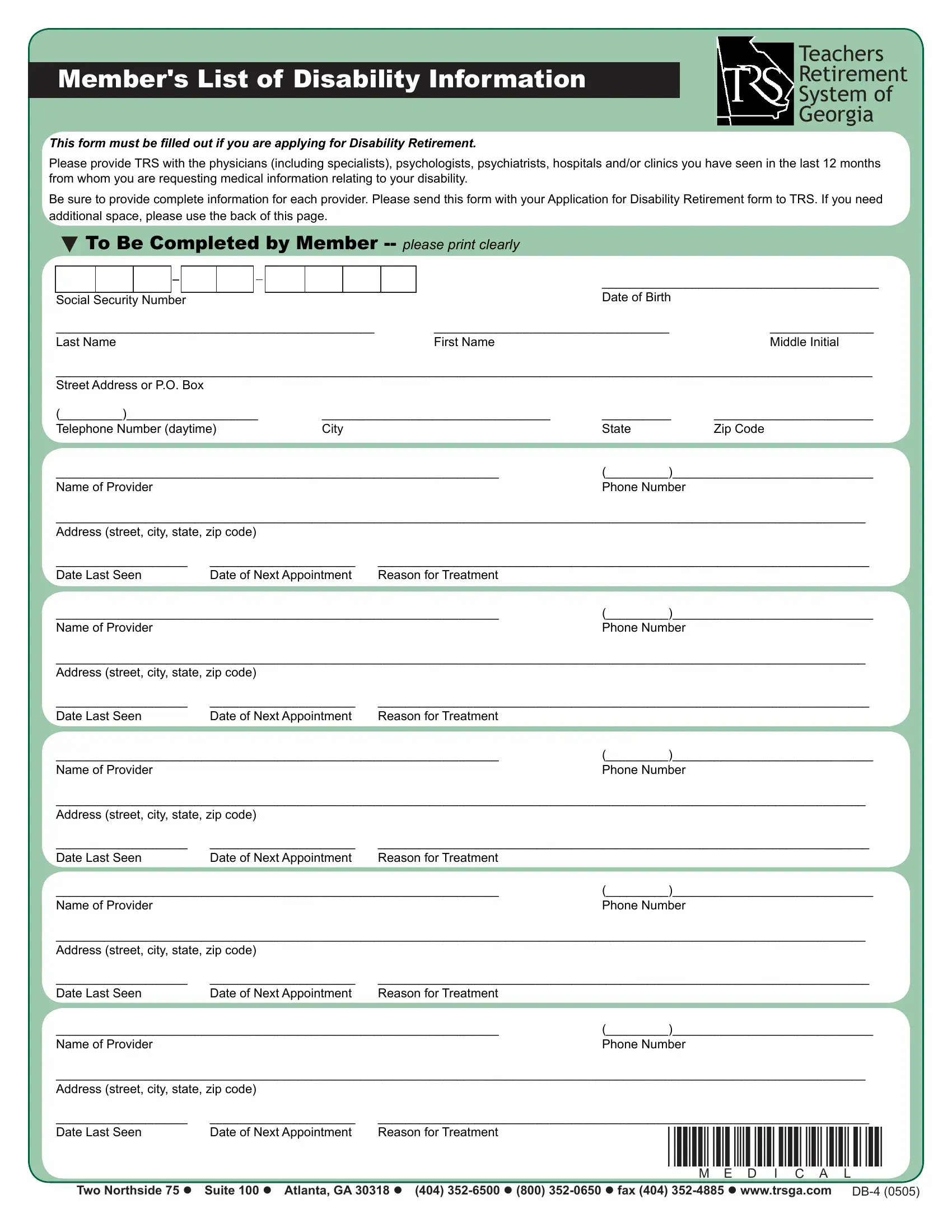
Member's List of Disability Information
This form must be illed out if you are applying for Disability Retirement.
Teachers
Retirement
System of
Georgia
Please provide TRS with the physicians (including specialists), psychologists, psychiatrists, hospitals and/or clinics you have seen in the last 12 months from whom you are requesting medical information relating to your disability.
Be sure to provide complete information for each provider. Please send this form with your Application for Disability Retirement form to TRS. If you need additional space, please use the back of this page.
To Be Completed by Member
|
|
|
|
|
|
|
|
|
|
|
|
________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Date of Birth |
|
Social Security Number |
|
||||||||||||
______________________________________________ |
|
__________________________________ |
_______________ |
||||||||||
Last Name |
First Name |
Middle Initial |
|||||||||||
______________________________________________________________________________________________________________________
Street Address or P.O. Box
(_________)___________________ |
_________________________________ |
__________ |
_______________________ |
Telephone Number (daytime) |
City |
State |
Zip Code |
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
Phone Number |
|
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
|
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
|
Phone Number |
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
|
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
|
Phone Number |
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
|
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
|
Phone Number |
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
|
________________________________________________________________ |
(_________)_____________________________ |
||
Name of Provider |
|
|
Phone Number |
_____________________________________________________________________________________________________________________
Address (street, city, state, zip code)
___________________ |
_____________________ |
_______________________________________________________________________ |
|
Date Last Seen |
Date of Next Appointment |
Reason for Treatment |
*MEDICAL* |
|
|||
Two Northside 75 Suite 100 Atlanta, GA 30318 (404)