
When using the online tool for PDF editing by FormsPal, it is easy to fill in or alter Porencephalic right here. The editor is constantly updated by us, receiving additional functions and turning out to be greater. Getting underway is effortless! Everything you need to do is stick to these basic steps directly below:
Step 1: Press the orange "Get Form" button above. It will open up our pdf tool so that you could begin filling out your form.
Step 2: With the help of our state-of-the-art PDF editor, you can accomplish more than merely fill out blank form fields. Try all of the features and make your documents seem high-quality with customized text put in, or optimize the file's original content to perfection - all that supported by the capability to incorporate your personal photos and sign the file off.
This document will need particular data to be filled out, hence be certain to take the time to enter what's requested:
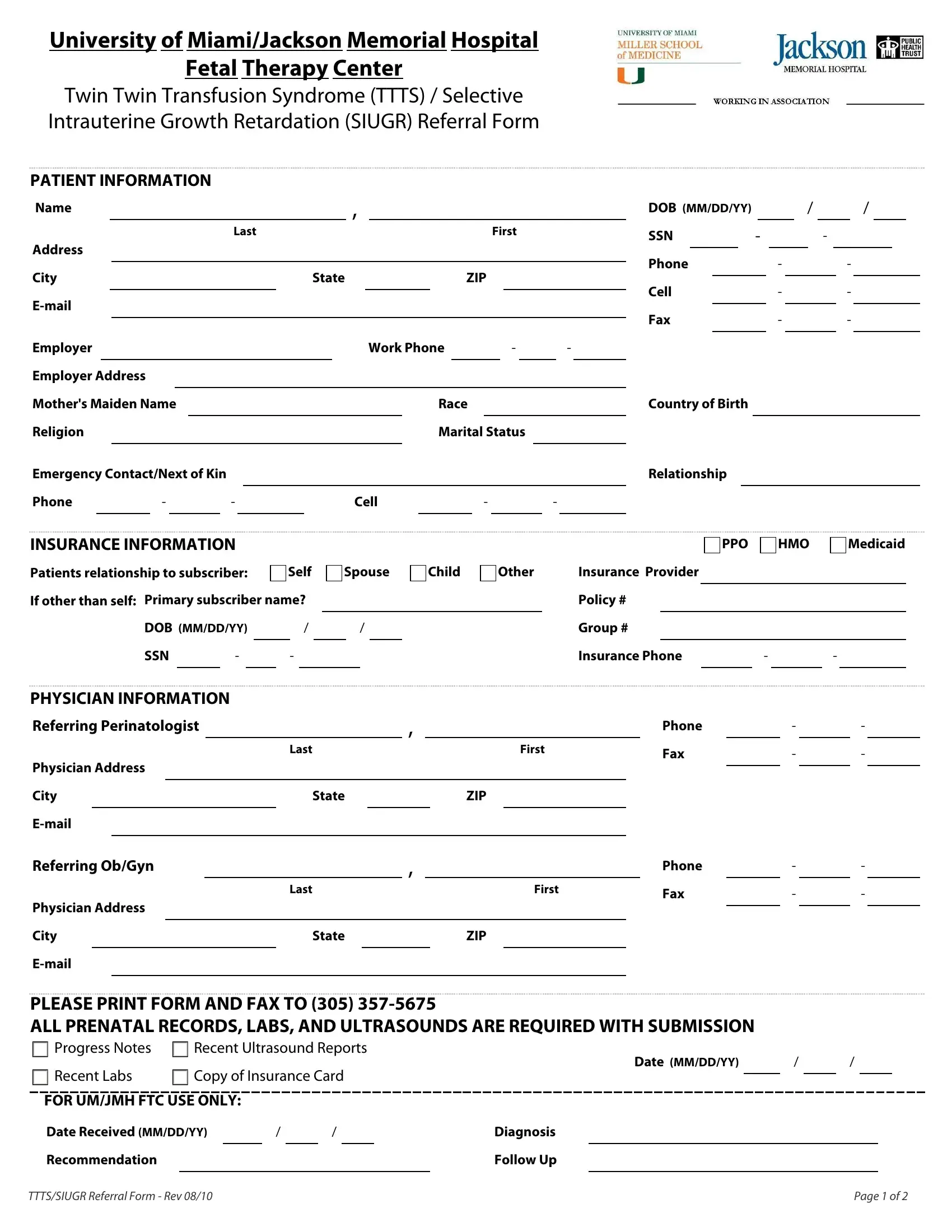
1. To start off, when completing the Porencephalic, start in the page that features the next fields:
2. Just after the prior part is completed, go to type in the applicable information in these - Referring Perinatologist, Physician Address, City, Email, Referring ObGyn, Physician Address, City, Email, Last, State, First, ZIP, Last, First, and State.
Always be extremely careful when filling in State and Physician Address, as this is where a lot of people make a few mistakes.
3. This third stage is simple - complete all of the empty fields in Recommendation, TTTSSIUGR Referral Form Rev, Follow Up, and Page of to complete the current step.

4. Completing DATE MMDDYY, AGE, GRAV, PARITY, LMP, EDC, GA weeks, days, Twins, Triplets, Maternal Weight, lbs, Placental Location, Anterior, and Fundal is essential in the fourth stage - make sure to take the time and fill out each and every blank!
5. This form must be finalized with this particular section. Below one can find a full list of form fields that need specific information for your document submission to be faultless: Yes, Yes, Genetic Screening, NT Screen, Quad screen ONTD, Down Syndrome, Down Syndrome, Yes, Yes, Yes, Yes, Yes, Yes, Yes, and Yes.
Step 3: Prior to finalizing the form, check that all blanks are filled out the proper way. When you think it's all fine, click on “Done." Right after setting up afree trial account at FormsPal, it will be possible to download Porencephalic or send it via email directly. The PDF file will also be at your disposal through your personal account with your modifications. FormsPal guarantees your data privacy with a secure system that never records or distributes any type of personal data used in the form. Feel safe knowing your files are kept protected when you use our tools!