Va Uai forms are an essential part of the process when applying for a loan in Brazil. While they can seem intimidating at first, these forms provide an effective way to make sure lenders have all of the necessary information needed to assess your application accurately and fairly. This blog post will provide an overview on Va Uai forms, what they are and how they fit into the loan application process. Here’s everything that you need to know about Va Uai as a borrower!
| Question | Answer |
|---|---|
| Form Name | Va Uai Form |
| Form Length | 12 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min |
| Other names | virginia uniform assessment instrument, certification uai, what is a uai online, virginia uai form |
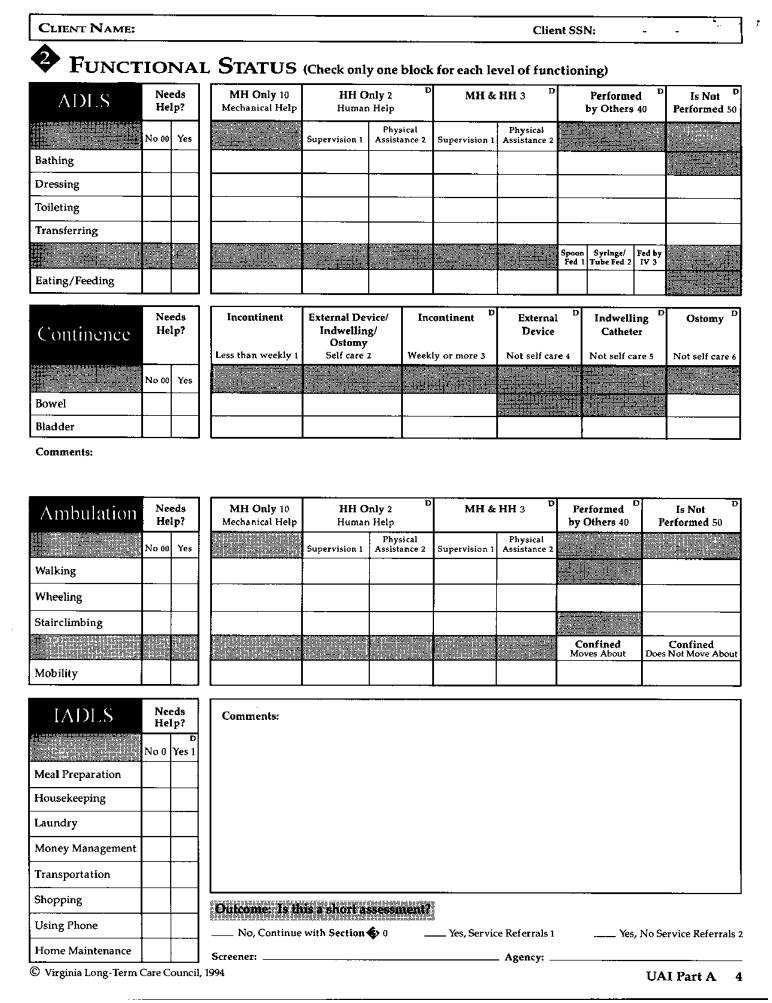
VIRGINIA UNIFORM ASSESSMENT INSTRUMENT
IDENTIFICATION/BACKGROUND
Dates: Screen |
/ |
AssessmentReassessment __ /
Client |
Name: |
|
|
Client |
SSN: |
|
|
|
(Last) |
(First) |
(Mlddle ImtlaI) |
|
|
Address: |
|
|
|
|
|
|
|
|
(Street) |
|
(City) |
(State) |
(Zip Code) |
Phone: |
( |
) |
|
City/County |
Code: |
|
Directions |
|
to House: |
|
|
Pets? |
|
Birthdate: |
|
/ |
/ |
|
Age: |
|
|
|
Sex: |
__ |
Male |
0 __ Female |
1 |
(Month) |
(Day) |
|
(Year) |
|
|
|
|
|
|
|
|
|
|
Marital Status: |
__ |
Married |
0 |
__ Widowed 1 |
__ |
Separated |
2 |
Divorced |
3 |
__ |
Single 4 |
Unknown 9 |
|
Race: |
|
|
|
Education: |
|
|
|
Communication of Needs: |
|
||||
White 0 |
|
|
|
Less than High School 0 |
Verbally,Enghsh 0 |
|
|||||||
Black/African |
American 1 |
|
Some |
High |
School 1 |
|
Verbally, |
Other |
Language 1 |
|
|||
American Indian |
2 |
|
High |
School |
Graduate |
2 |
Specify |
|
|
|
|||
Oriental/Asian |
3 |
|
|
Some |
College |
3 |
|
Sign Language/Gestures/Device |
2 |
||||
Alaskan Native 4 |
|
|
College Graduate 4 |
|
Does Not Commumcate 3 |
|
|||||||
Unknown9 |
|
|
|
Unknown9 |
|
|
HearingimpalredP |
|
|
||||
EthnicOrigin |
|
|
|
Specify |
|
|
|
|
|
|
|
|
|
Name: |
Relationship: |
|
Address: |
Phone:(H) |
(W) |
Name: |
Relationship: |
|
Address: |
Phone:(H) |
tW) |
Name of Primary Physician: |
Phone: |
|
Address: |
|
|
Who called:
(Name)(RelahontoChent)(Phone)
Presenting Problem/Diagnosis:
© |
UAl Part A 1 |
I CLIENTNAME: |
ClientSSN: |
- |
No 0 Yes 1 |
CheckAll |
Servzces That Apply |
Provider/Frequency: |
||||
|
Adu]t |
Day |
Care |
|
|
|
|
|
Adult |
Protective |
|
|
|
||
|
Case Management |
|
|
|
|||
|
Chore/Companion/Homemaker |
|
|
||||
|
Congregate |
|
Meals |
/ Senior |
Center |
|
|
|
Financial |
Management/Counseling |
|
||||
|
Friendly |
Visitor/Telephone |
Reassurance |
|
|||
|
Habfiltatlon/Supported |
Employment |
|
||||
|
Home |
Delivered |
Meals |
|
|
||
|
Home |
Health/Rehabilitation |
|
|
|||
|
Home |
Repalrs/Weatherizatlon |
|
||||
|
Housing |
|
|
|
|
|
|
|
Legal |
|
|
|
|
|
|
|
Mental Health (Inpatient/Outpatient) |
|
|||||
|
Mental |
Retardation |
|
|
|
||
|
Personal |
Care |
|
|
|
||
|
Respite |
|
|
|
|
|
|
|
Substance |
|
Abuse |
|
|
|
|
Transportation
Vocational Rehab/Job Counseling
Other
$20,000or More ($1,667orMore)0 |
|
No 0 |
Yes 1 |
|
|
|
|
|
Names |
||||||||
$15,000 - $19,999 ($1,250 - $1,666) 1 |
|
|
Legal |
Guardian, |
|
|
|
||||||||||
$11,000 - $14,999 ($ |
917- |
$1,249) |
2 |
|
|
Power |
of |
Attorney, |
|
|
|||||||
$ 9,500 - $10,999 ($ |
792 |
- $ |
916) |
3 |
|
|
Representative |
Payee, |
|
|
|||||||
$ |
9,499($ |
583- |
$ |
791)4 |
|
|
|
Other, |
|
|
|
|
|
|
|||
$ |
|
6,999($ |
582) |
5 |
|
|
|
|
|
|
|
|
|
||||
$ |
5,499 or |
Less |
($ |
457 |
or |
Less) |
6 |
|
Do your4_q_ve anybenefi_ |
_fifi_? |
|
|
|||||
Unknown9 |
|
|
|
|
|
|
No 0 |
Yes1 |
|
|
|
|
|
|
|||
Numberin Familyunit. |
|
|
|
|
|
|
AuxiliaryGrant |
|
|
||||||||
Optional. |
Total monthly farmly income |
|
|
|
|
Food |
Stamps |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
Fuel |
Assistance |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
General |
Relief |
|
|
|
||
DO yOU |
currently receive |
income |
from.,. |
? |
|
State |
and |
Local |
Hospltahzatlon |
||||||||
No 0 Yes 1 |
|
|
|
|
|
Optwnal |
Amount |
|
Subsidized |
Housing |
|
|
|||||
|
Black Lung, |
|
|
|
|
|
|
Tax Relief |
|
|
|
|
|||||
|
Pension, |
|
|
|
|
|
V_/hat |
insurance |
do |
you |
have? |
||||||
|
Social |
Security, |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
SSI/SSDI, |
|
|
|
|
|
No 0 |
Yes |
|
|
|
|
|
|
|||
|
VA Benefits, |
|
|
|
|
|
|
Medicare, |
|
# |
|
|
|
||||
|
Wages/Salary, |
|
|
|
|
|
|
Medicaid, |
|
# |
|
|
|
||||
|
Other, |
|
|
|
|
|
|
|
Pending |
|
_ No |
0 _1 |
Yes |
||||
QMB/SLMB |
[] No 0 [] |
Yes |
All Other Public/Private |
|
|
© Virginia |
|
UA1 Part A 2 |
CLIENTNAME: |
ClientSSN: |
- |
Where do you usually live? Does anyone live with you?
Alone 1 |
Spouse 2 |
Other 3 |
Names of Persons in Household |
HouseOwn0
House Rent 1
House Other 2
i
Apartment 3
Rented Room 4
|
|
Name of Provider |
Admission |
Provider Number |
|
|
(Place) |
Date |
(IfApphcable) |
AdultCareResldence50 |
|
I |
||
Adult Foster |
60 |
|
|
|
Nursing |
Facfilty 70 |
|
|
|
Mental |
Health/ |
|
|
|
Retardation |
Facility 80 |
|
|
|
|
|
|
|
I |
Other |
90 |
|
|
l |
|
|
|
||
No 0 Yes l |
Check All Problems That Apply |
Describe |
Problems: |
Barriers to Access
Electrical Hazards
Fire Hazards/No Smoke Alarm
Insufficient Heat/Air Conditioning
Insufficient Hot Water/Water
Lack of/Poor Toilet Facilities (Inside/Outside)
Lack of/Defective Stove, Refrigerator, Freezer
Lack of/Defective Washer/Dryer
Lack of/Poor Bathing Faclhtles
Structural Problems
Telephone Not Accessible
Unsafe Neighborhood
Unsafe/Poor Lighting
Unsanitary Conditions
Other:
© |
UAI Part A 3 |
I CI'.IENTNAME: |
ClientSSN: |
- |
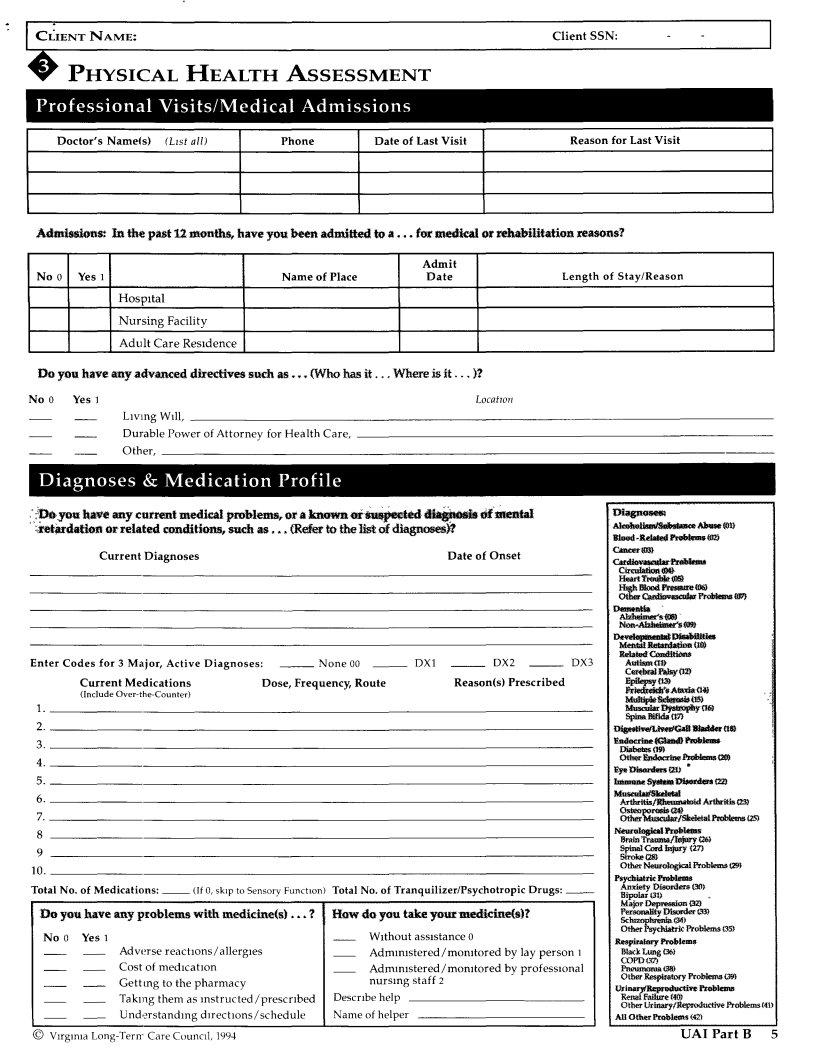
PHYSICAL HEALTH ASSESSMENT
|
|
|
I |
|
Doctor's Name_s) |
(L_st all) |
Phone |
Date of Last Visit |
Reason for Last Visit |
Admissions.- In the past i2 months, have you been admired to a ,.. for medical or rehabfiitation reasons?
|
|
Admit |
|
No 0 Yes 1 |
Name of Place |
Date |
Length of Stay/Reason |
Hospital |
|
|
|
NursingFacility |
|
! |
|
Adult Care Residence |
|
|
|
Do |
you have any advanced directives such as... (Who has it.., Where is it.., |
)? |
No0 |
YesI |
Locatwn |
|
Living Wdl, |
|
|
Durable Power of Attorney for Health Care, |
|
|
Other, |
|
;?_,y(m |
have |
any current medical |
problems, |
or a _or |
_i_tearl |
_i_,_ |
_ |
meltial |
|
|
|
D'_osem |
|
|
|
|||||
_lr_dation |
or related |
conditmns, |
such as,** |
(Refer |
to the |
llst of diagnoses_ |
|
|
|
|
|
: _ |
'__0_ |
!'roMt,m_ |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
slooa |
|
|||
|
|
CurrentDiagnoses |
|
|
|
|
|
DateofOnset |
|
|
|
_ |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cat_1_tar_ulat_ |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C_reulattca_ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H_a't_nml_ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i |
|
|
|
|
Enter Codes for |
3 Major, |
Active Diagnoses: |
__ |
None 00 __ |
DX1 |
__ |
DX2 |
__ |
|
DX3 |
|
Au_ismlt_ |
|
|
||||||
|
|
Current Medications |
|
Dose, Frequency, |
Route |
|
Reason(s) Prescribed |
|
|
|
Elvlk'P_i_ |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
_i_Ataltat |
¢f_ |
.: |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__._ |
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_l_ac, |
|
cal_ |
tt_ |
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_ulo_a_na_ |
|
|
||
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Er._ |
|
;n) ' |
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
lmmu_ S_ |
Dl_a*a_*s |
|||
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_hat, |
|
tal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Azhkrttlsl |
.Rlmmna_d A.*flu4tis |
||
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Osmoporosi_sa0 |
eaaaemsc2_ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ot_l_luKtaatt_l |
||||
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N_roIo_i_t_bbmu |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Brain Tra_n_/_ |
126) |
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stroke_ |
|
|
|
10. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OtherNatr_Pr_lems |
tz_ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Psychia_rki_al_m |
|
|||
Total |
No. of Medications: |
(If 0, skip to Sensory |
Function) Total |
No. of Tranquilizer/Psychotropic |
Drugs: |
|
|
Anxiety Diaord_rO0)s |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bipolar |
(3D |
., |
|
||
Do |
you |
have any p_oblems |
with |
medicine(s). |
? |
How |
do you take your medicine(s)? |
|
|
|
|
P_r_ |
_m_ |
|
||||||
No 0 |
Yes1 |
|
|
|
|
|
|
W_thoutassistance0 |
|
|
|
|
|
Psyckla feProblemTs35) |
||||||
|
|
|
|
|
|
|
|
|
|
R_pir_ _b_m |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Adw_'rse reactions/allergies |
|
|
Admm_stered/momtored |
by lay person |
1 |
|
__ |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COPD_3_ |
|
|
|
|
|
|
Cost of me&cat_on |
|
|
|
Admm_stered/momtored |
by professional |
|
|
P_m) |
|
|
|
||||||
|
|
|
Gettmg |
to the |
pharmacy |
|
|
nursing |
staff 2 |
|
|
|
|
|
|
ot_s__09_ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ttsri_!m_twav_ l'r_ |
||||
Taking
CLIENT NAME:Client SSN:]
iiiiiiiiiiiiiii i ii i |
iii! iiii! |
ili |
i ii!iiiiiiiiiiiiiiiii!i!iiiiiiii |
|
|
||
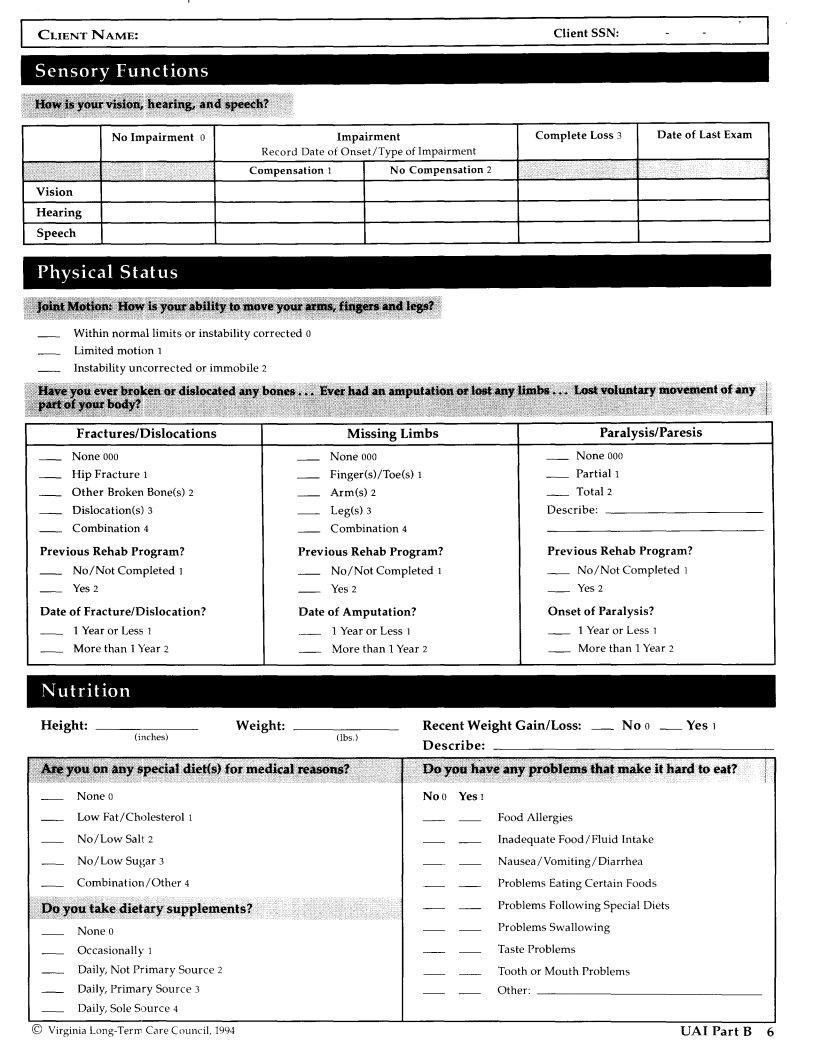
|
No Impairment |
0 |
|
|
Impairment |
Complete Loss 3 |
Date of Last Exam |
|
|
|
Record Date |
of Onset/Type of Impairment |
|
|
|
|
|
|
Compensation |
1 |
No Compensation |
2 |
|
Vision |
|
|
|
|
|
|
|
Hearing |
|
|
|
|
|
|
|
Speech |
|
|
|
|
|
i |
|
Within normal limits or instability corrected 0 |
|
|
|
||||
Limited |
motion 1 |
|
|
|
|
||
Instability uncorrected or immobile 2 |
|
|
|
|
|||
:::::.::. :;=.I |
I |
I III: |
I |
II |
I |
I |
_, |
Fractures/Dislocations |
Missing Limbs |
|
Paralysis/Paresis |
||||
None000 |
|
None000 |
__ |
None000 |
|
||
Hip |
Fracture |
1 |
Finger(s)/Toe(s) 1 |
__ |
Partial 1 |
|
|
OtherBrokenBone(s)2 |
Arm(s)2 |
__ |
Total2 |
|
|||
Dislocation(s)3 |
Leg(s)3 |
Describe: |
|
||||
Combination4 |
Combination4 |
|
|
|
|||
Previous |
Rehab Program? |
Previous Rehab Program? |
Previous Rehab |
Program? |
|||
No/Not Completed 1 |
No/Not Completed ] |
__ |
No/Not Completed ] |
||||
Yes2 |
|
|
Yes2 |
__ Yes2 |
|
||
Date of Fracture/Dislocation? |
Date of Amputation? |
Onset |
of Paralysis? |
||||
1Yearor Less1 |
1YearorLess1 |
|
1YearorLess |
||||
Morethan 1Year2 |
Morethan 1Year2 |
__ |
Morethan 1Year2 |
||||
Height: |
Weight: |
Recent Weight Gain/Loss: |
No 0 __ Yes |
(inches) |
|
(lbs.) |
|
|
|
Describe: |
|
None0 |
|
No0 Yes1 |
|
Low Fat/Cholesterol |
] |
Food Allergies |
|
|||
No/Low |
Salt 2 |
|
|
Inadequate |
Food/Fluid |
Intake |
No/Low |
Sugar |
3 |
|
Nausea/Vomiting/Diarrhea |
|
|
Combination/Other |
4 |
Problems |
Eating Certain |
Foods |
||
|
|
|
|
Problems |
Following Special Diets |
|
None0 |
|
|
|
ProblemsSwallowing |
||
Occasionally1 |
|
TasteProblems |
|
|||
Daily, Not Primary |
Source 2 |
Tooth or |
Mouth Problems |
|||
Daily, Primary |
Source 3 |
Other: |
|
|
||
Daily, Sole Source 4 |
|
|
|
|
||
© Virginia |
|
|
UA1 Part B 6 |
|||
'! C IENTNAME |
C,ientSSN: I |
iiiiiiiiii |
i_ii_ |
i |
i!iiii!iiii!¸¸ |
iiiiii!ii!i |
_i_i_!_i_i_i!ii!!i_i_ii_iiiii!!_i_!i!ii_!i_! |
||
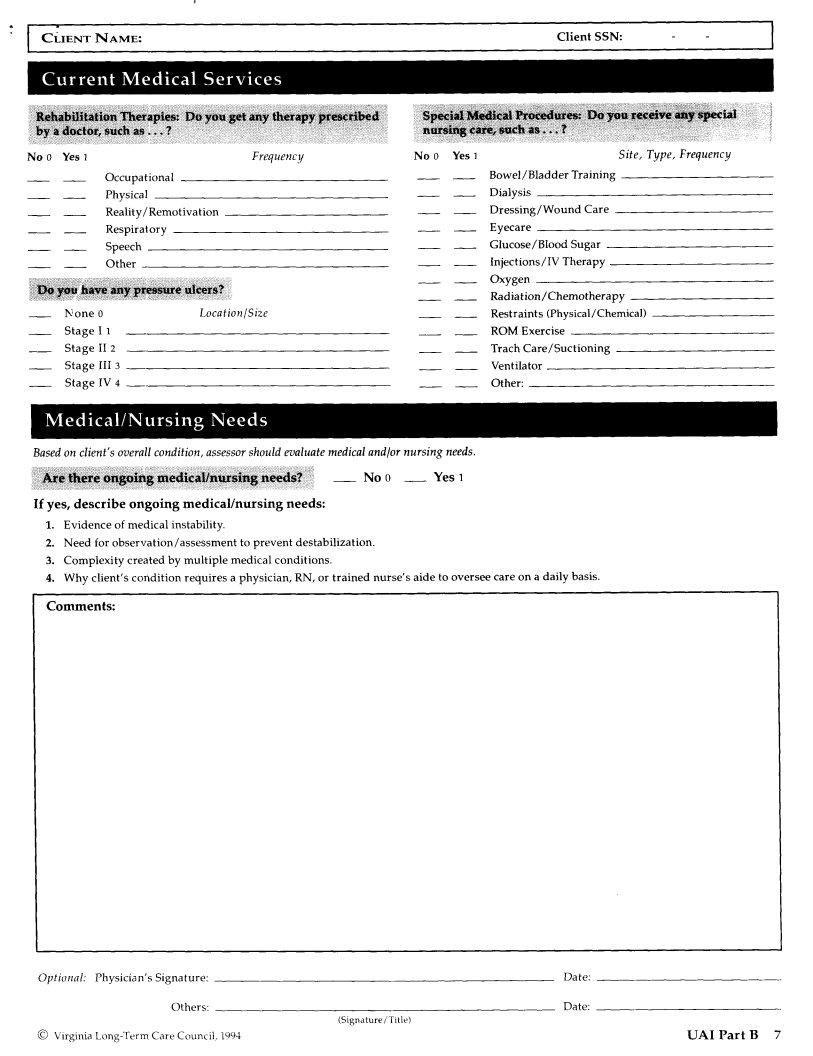
No 0 Yes 1 |
Frequency |
No 0 Yes 1 |
Occupational
Physical
Reality/Remotivation
Respiratory
Speech
Other
None |
0 |
Location/Size |
Stage |
I |
1 |
Stage |
II 2 |
|
StageIII3
StageIV4
Based on client's overall condition, assessor should evaluate medical and/or nursing needs.
__ No 0 __ Yes 1
If yes, describe ongoing medical/nursing needs:
1.Evidence of medical instability.
2.Need for observation/assessment to prevent destabilization.
3.Complexity created by multiple medical conditions.
4.Why client's condition requires a physician, RN, or trained nurse's aide to oversee
Comments:
Site, Type, Frequency
Bowel/Bladder Training
Dialysis
Dressing/Wound Care
Eyecare
Glucose/Blood Sugar
Injections/IV Therapy
Radiation/Chemotherapy
Restraints (Physical/Chemical)
ROM Exercise
Trach Care/Suctioning
Ventilator
Other:
care on a daily basis.
Optional: |
Physician's |
Signature: |
Date: |
|
|
Others: |
Date: |
|
|
|
(Signature / Title) |
(_ Virginia |
Care Council, 1994 |
UAI Part B 7 |
CLIENTNAME: |
ClientSSN: |
I |
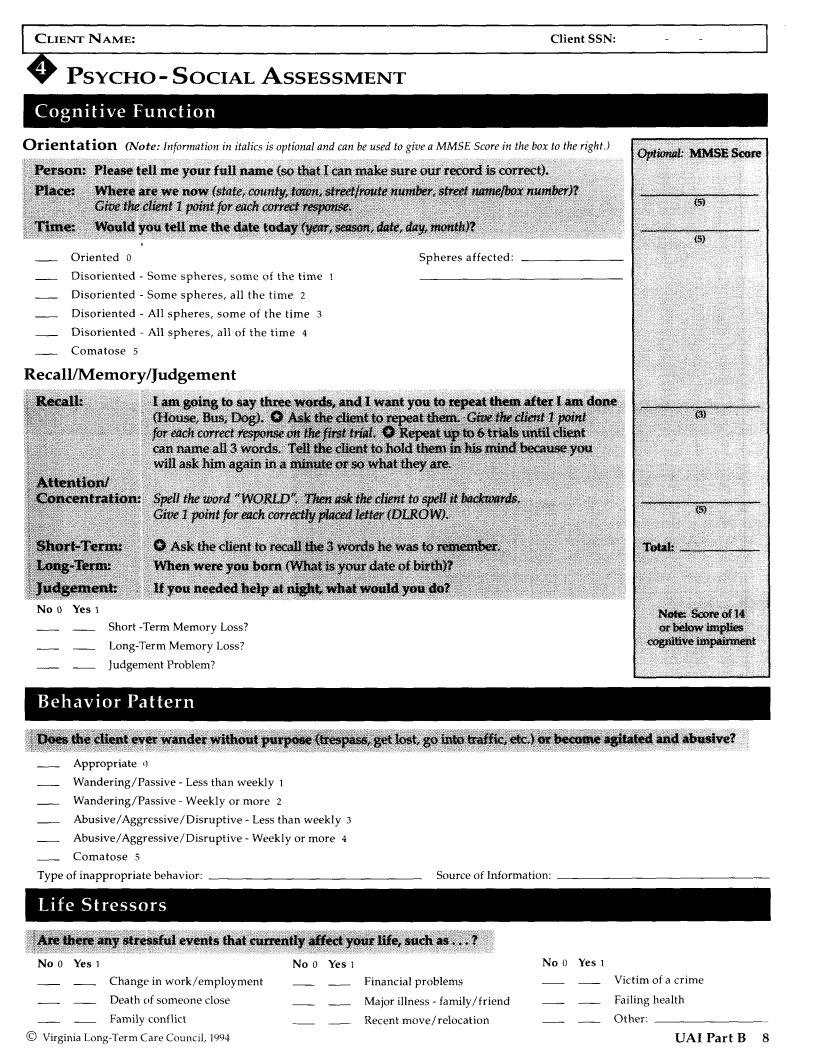
PSYCHO- SOCIAL ASSESSMENT
Orientation (Note: Information in italics is optional and can be used to give a MMSE Score in the box to the right.)
Oriented0 |
Spheresaffected: |
Disoriented - Some spheres, some of the time 1
Disoriented - Some spheres, all the time 2
Disoriented - All spheres, some of the time 3
Disoriented - All spheres, all of the time 4
Comatose 5
Recall/Memory/Judgement
No 0 Yes I
Short
Judgement Problem?
i _ _iii_ilEii!iiiiiii_iiiii??iiii!iiiiiiii?Z:* iiii ii!iiiiiiili!ii_iiiiii!ili!iiiii!ilili!i!iiiiiiiiiiiiiii!iiiiiiii?iiiii!i: : [ : iiiiii?i!i!ii_i_i_i_i_i!?_ii_i!?_i_i!ii_!_i_!ii_ii?_i?_!_!_i_i_i_i_i_i!i_i_i_iii_i?_?_i_!_ii?ii_i!i
Appropriate |
0 |
|
|
|
|
Wandering/Passive |
- Less than weekly 1 |
|
|||
Wandering/Passive |
- Weekly or more |
2 |
|
||
Abusive/Aggressive/Disruptive |
- Less |
than weekly |
3 |
||
Abusive/Aggressive/Disruptive |
- Weekly or more |
4 |
|||
Comatose |
5 |
|
|
|
|
Typeof inappropriate behavior: |
|
|
Sourceof Information: |
||
No0 YesI |
|
No0 Yes1 |
No0 Yesl |
|
Change |
in work/employment |
Financial problems |
Victim |
of a crime |
Death |
of someone close |
Major illness - family/friend |
Failing |
health |
Family |
conflict |
Recent move/relocation |
Other: |
|
© Virginia |
|
|
UAI Part B 8 |
|
CLIENTNAME: |
ClientSSN: |
|
|
|
|
|
|
|
|
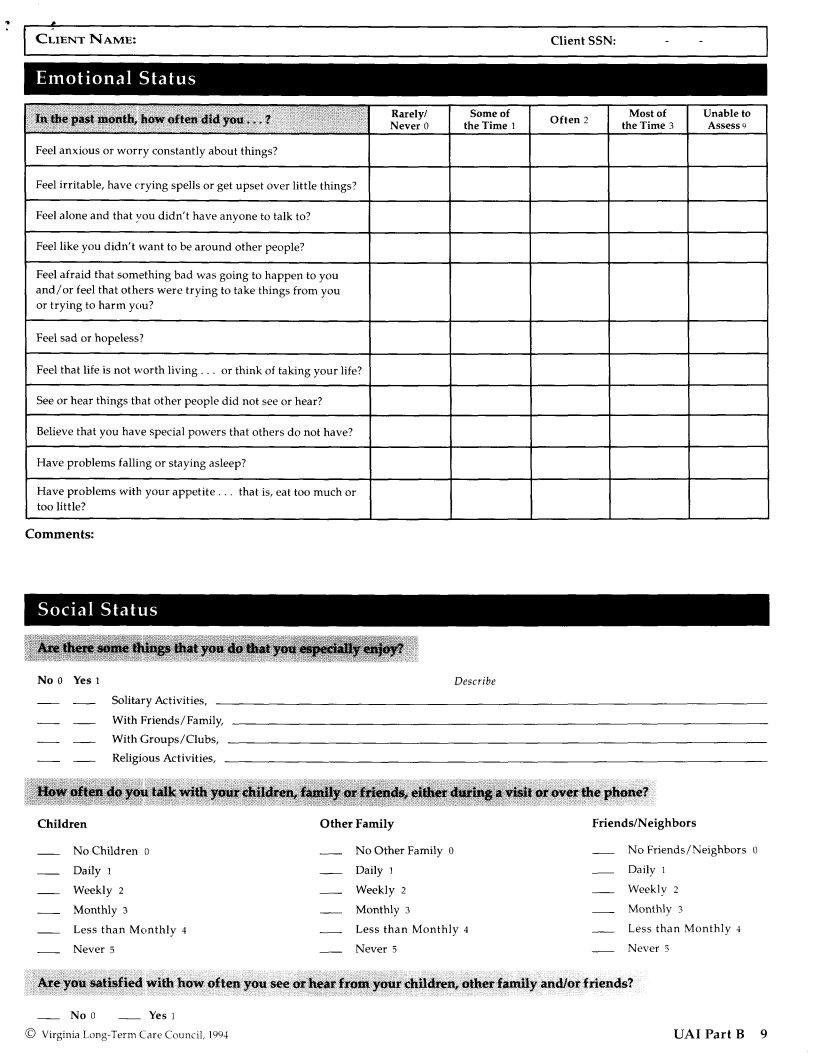
Rarely/ |
Some of |
Often 2 |
Most of |
Unable to |
l |
|
|
|
|
|
|
|
|
Never0 |
theTime 1 |
|
theTime3 |
Assess9 |
|
Feel anxious or worry constantly about things? |
|
|
|
|
|
|
|
||||||
Feel irritable, have crying spells or get upset over little things? |
|
|
|
|
|
||||||||
Feel alone and that you didn't have anyone to talk to? |
|
|
|
|
|
|
|
||||||
Feel like you didn't want to be around other people? |
|
|
|
|
|
|
|
||||||
Feel afraid that something bad was going to happen to you |
|
|
|
|
|
|
|||||||
and/or feel that others were trying to take things from you |
|
|
|
|
|
|
|||||||
or trying to harm you? |
|
|
|
|
|
|
|
|
|
|
|||
Feel |
sad |
or hopeless? |
|
|
|
|
|
|
|
|
|
|
|
Feel |
that |
life is not worth |
living.., |
or think |
of taking |
your |
life? |
|
|
|
|
|
|
See or hear things that other people did not see or hear? |
|
|
|
|
|
|
|||||||
Believe that you have special powers that others do not have? |
|
|
|
|
|
||||||||
Have problems |
falling or staying asleep? |
|
|
|
|
|
|
|
|
||||
Have |
problems |
with your |
appetite.., |
that |
is, eat too |
much |
or |
|
|
|
|
|
|
toolittle? |
|
|
|
|
|
|
|
I |
|
|
|
||
Comments:
No0 Yes1 |
Describe |
Solitary Activities,
With Friends/Family,
With Groups/Clubs,
Religious Activities,
Children |
Other Family |
Friends/Neighbors |
|
No Children 0 |
No Other Family 0 |
No Friends/Neighbors |
0 |
Daily1 |
Daily_ |
Daily |
|
Weekly2 |
Weekly2 |
Weekly2 |
|
Monthly3 |
Monthly3 |
Monthly3 |
|
Less than Monthly 4 |
Less than Monthly 4 |
Less than Monthly 4 |
|
Never5 |
Never5 |
Never5 |
|
No 0 |
Yes 1 |
|
|
(_) Virginia |
Care Council, 1994 |
UA1 Part g |
9 |
I CLIENT |
Client SSN: |
- |
ii!iliiiii _iii_iiiiiiiiiiiiiiiiii__iiiiiiiiiiiiii!iiii!1!iiiii _i_iigiiiiiiiiiiiiigiiiiiiiiiiiii!iiiiiiiiiiiiiiiiiii2i__iiiiiiiiiiiiiiiiiiiii_iiiziz_iziii_ii__iiii___i_i_i__iii_iigii_iiiiiiiii_i
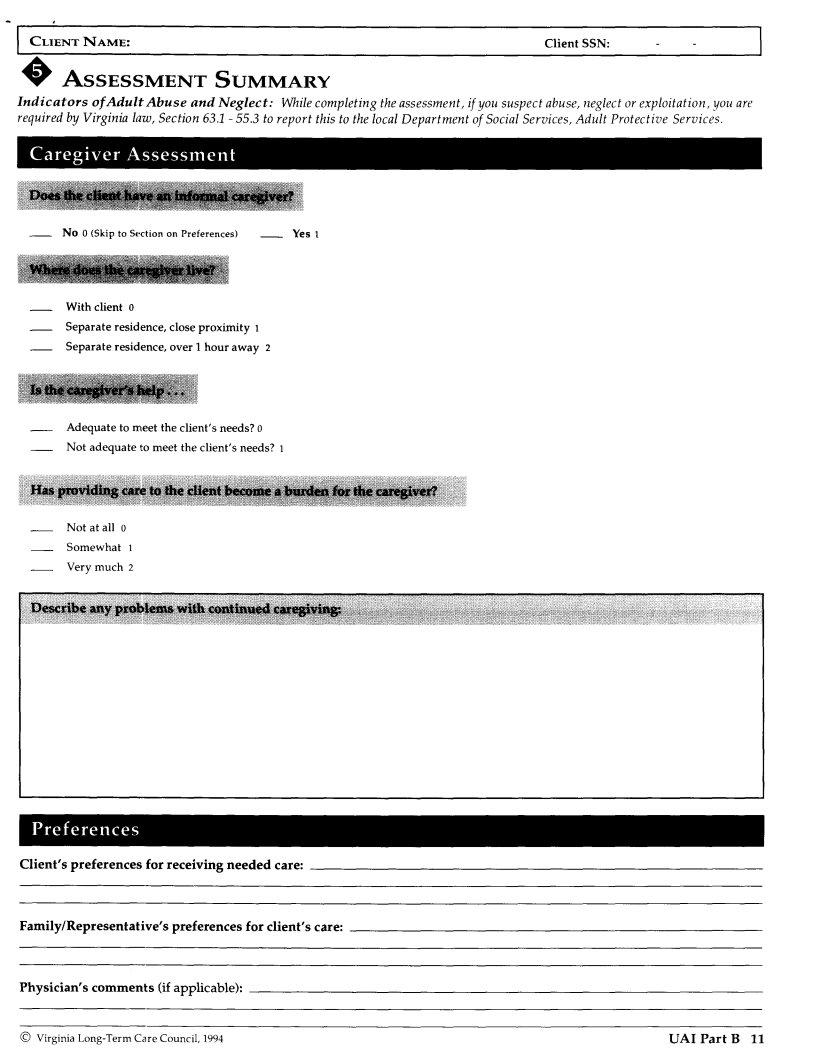
I CLIENTNAME:ClientSSN:
ASSESSMENT |
SUMMARY |
Indicators of Adult Abuse |
and Neglect: While completing the assessment, if you suspect abuse, neglect or exploitation, you are |
required by Virginia law, Section 63.1 - 55.3 to report this to the local Department of Social Services, Adult Protective Services.
No 0 (Skip to Section on Preferences) |
Yes l |
With client 0
Separate residence, close proximity 1
Separate residence, over 1 hour away 2
Adequate to meet the client's needs? 0
Not adequate to meet the client's needs? 1
Not at all 0
Somewhat 1
Very much 2
Client's preferences for receiving needed care:
Family/Representative's preferences for client's care:
Physician's comments (if applicable):
© Virginia |
UAI Part B 11 |
CLIENT NAME: |
Client SSN: |
- |
I |
No 0 Yes 1 (CheckAll That Apply) |
No 0 Yes 1 (CheckAll That Apply) |
|
||
Finances |
|
Assistive |
Devices/Medical |
Equipment |
Home/Physical |
Environment |
Medical |
Care/Health |
|
ADLS |
|
Nutrition |
|
|
IADLS |
|
Cognitive/Emotional |
|
|
|
|
Caregiver |
Support |
|
Assessor's Name |
Signature |
Agency/Provider |
Name |
Provider# |
Section(s) |
|
|
|
|
|
Completed |
Optional: |
Case assigned to: |
Code #: |
© Virginia |
UAI Part B 12 |