For prospective students considering the University of California, Los Angeles (UCLA), the Form 500575 is a key document. The form acts as an agreement between UCLA and new applicants that states all potential students must agree to abide by university policies and regulations once enrolled. While completing this step may seem daunting, it is an important part of the application process that you should take seriously in order to future proof your acceptance into one of America's top universities. In this blog post, we will provide information on what the UCLA Form 500575 entails and how it can help expedite your entreance to the school. So keep reading if you want to get up-to-speed on everything related to Form 500575!
| Question | Answer |
|---|---|
| Form Name | Ucla Form 500575 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | intake form ucla pdf, ucla kidney donor intake form, intake form ucla, donor intake form |
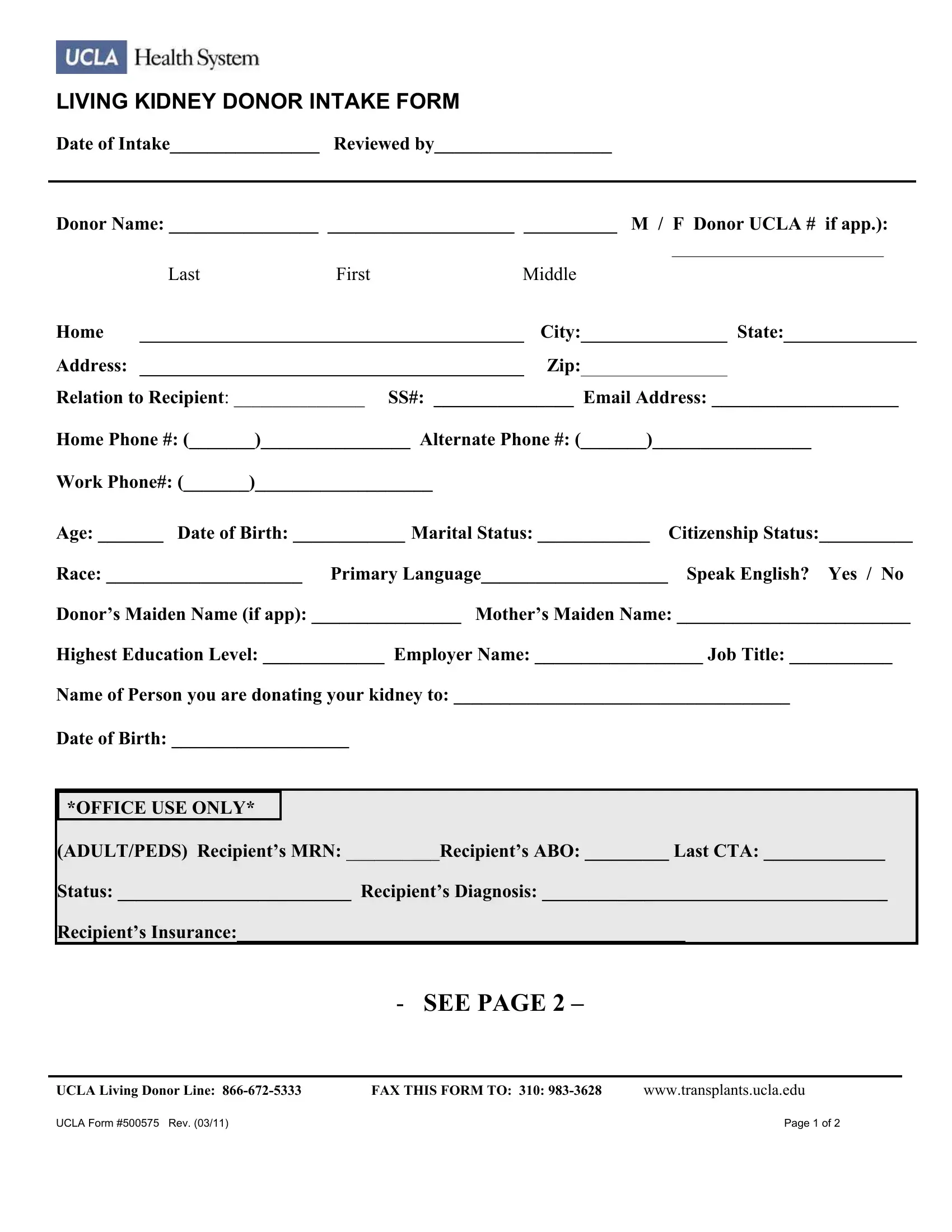
LIVING KIDNEY DONOR INTAKE FORM
Date of Intake________________ Reviewed by___________________
Donor Name: ________________ ____________________ __________ M / F Donor UCLA # if app.):
|
|
|
|
|
___________________________ |
||
|
Last |
First |
Middle |
|
|
|
|
Home |
|
|
City: |
|
State: |
||
|
|
|
|
|
|
|
|
Address: |
|
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
Relation to Recipient: ______________ SS#: _______________ Email Address: ____________________
Home Phone #: (_______)________________ Alternate Phone #: (_______)_________________
Work Phone#: (_______)___________________
Age: _______ Date of Birth: ____________ Marital Status: ____________ |
Citizenship Status:__________ |
Race: _____________________ Primary Language____________________ |
Speak English? Yes / No |
Donor’s Maiden Name (if app): ________________ Mother’s Maiden Name: _________________________
Highest Education Level: _____________ Employer Name: __________________ Job Title: ___________
Name of Person you are donating your kidney to: ____________________________________
Date of Birth: ___________________
*OFFICE USE ONLY*
(ADULT/PEDS) Recipient’s MRN: __________Recipient’s ABO: _________ Last CTA: _____________
Status: _________________________ Recipient’s Diagnosis: _____________________________________
Recipient’s Insurance:________________________________________________
- SEE PAGE 2 –
UCLA Living Donor Line: |
FAX THIS FORM TO: 310: |
www.transplants.ucla.edu |
UCLA Form #500575 Rev. (03/11) |
|
Page 1 of 2 |

LIVING KIDNEY DONOR INTAKE FORM
Donor’s ABO: __________ Ht: __________ Wt: __________
Medications (prescription and
Blood Sugar Problems (yourself or family): __________________________ During pregnancy? ____________
High Blood Pressure (yourself or family): ___________________________ During pregnancy? ____________
Heart Problems (yourself or family): ____________________________________________________________
Any history of melanoma?: __________ If yes, how long ago were you diagnosed?: _____________________
Kidney Stones or Kidney Problems (yourself or family): ____________________ Cancer: ________________
Urine or Kidney Infections: ___________________________ Liver Problems or Hepatitis:________________
Alcohol / Tobacco/Drug Use: ________________________ Mental Health Problems: ____________________
Hospitalizations/Surgeries/Other Health Problems: ________________________________________________
Any bleeding problems? _____________________________________________________________________
Have you been
Have you ever been incarcerated, and if so how long ago? __________________________________________
When was your latest: Pap Smear (Females only) ___________ Mammogram (Females > 40) ______________
Colonoscopy ( > 60) _______________
Have you discussed your intention to donate with your family/significant other? _________________________
Do you have health insurance? _______Who will take care of you after the surgery? _____________________
Signature of Donor _________________________________________________ Date ________________
Signature of Person Filling Out
Report (if other than donor) |
|
Print Name |
Date ______________ |
UCLA Living Donor Line: |
FAX THIS FORM TO: 310: |
www.transplants.ucla.edu |
UCLA Form #500575 Rev. (03/11) |
|
Page 2 of 2 |