
Dealing with PDF documents online is surprisingly easy with this PDF tool. You can fill out direct deposit 160 here within minutes. To retain our editor on the cutting edge of efficiency, we aim to adopt user-oriented capabilities and improvements regularly. We are routinely looking for feedback - play a pivotal role in revolutionizing PDF editing. With a few easy steps, you may begin your PDF editing:
Step 1: Access the PDF file in our tool by clicking the "Get Form Button" in the top part of this webpage.
Step 2: Using our advanced PDF tool, you can actually do more than merely fill out blank fields. Try all of the functions and make your documents appear great with customized text incorporated, or fine-tune the original content to perfection - all comes along with the capability to add stunning pictures and sign the file off.
This PDF form requires particular details to be typed in, so be sure you take whatever time to provide precisely what is required:
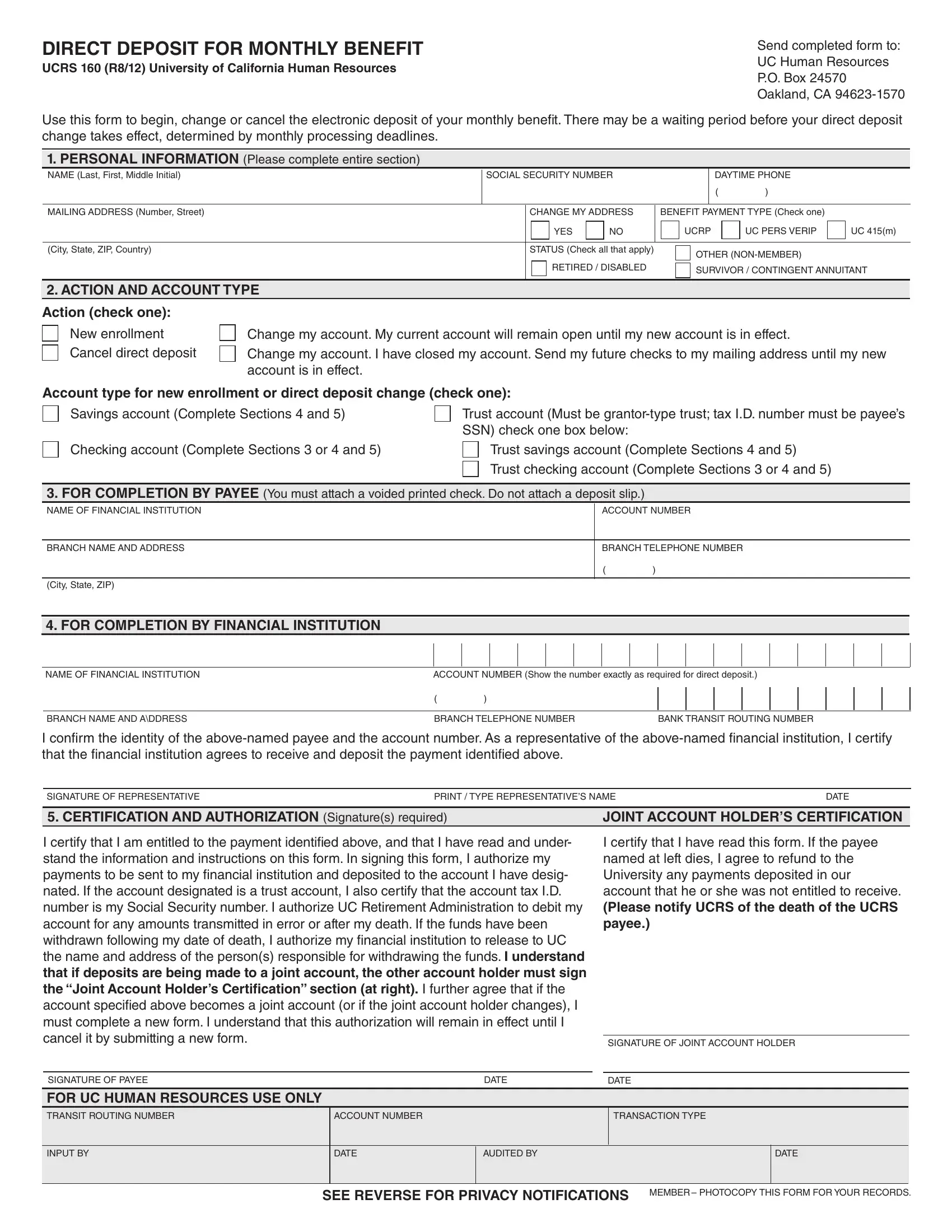
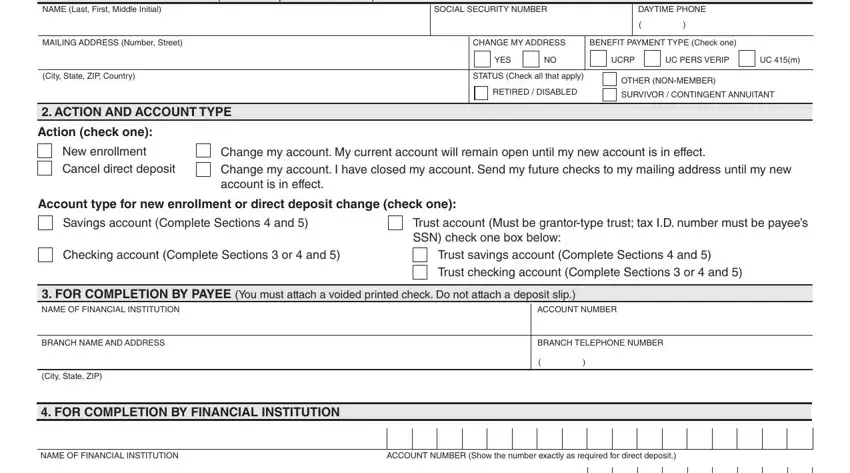
1. When submitting the direct deposit 160, make sure to complete all of the needed fields within the associated form section. This will help to hasten the work, allowing for your information to be processed without delay and appropriately.
2. After this array of fields is finished, it's time to insert the required specifics in BRANCH NAME AND ADDRESS, BRANCH TELEPHONE NUMBER, BANK TRANSIT ROUTING NUMBER, I conirm the identity of the, SIGNATURE OF REPRESENTATIVE, PRINT TYPE REPRESENTATIVES NAME, DATE, CERTIFICATION AND AUTHORIZATION, JOINT ACCOUNT HOLDERS CERTIFICATION, I certify that I am entitled to, I certify that I have read this, SIGNATURE OF JOINT ACCOUNT HOLDER, SIGNATURE OF PAYEE, DATE, and DATE allowing you to go further.
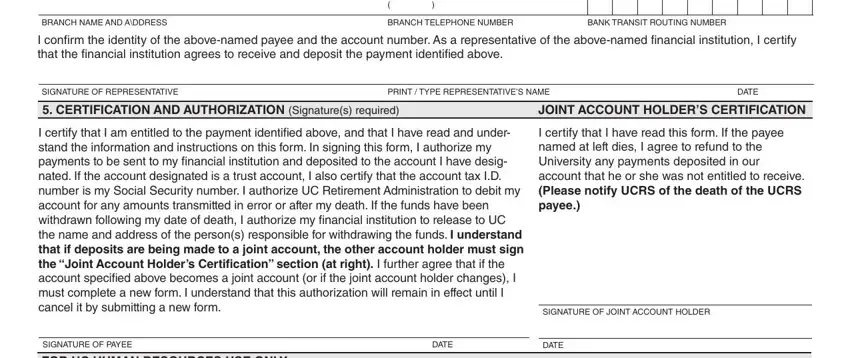
People often make mistakes while filling out BANK TRANSIT ROUTING NUMBER in this part. Be sure to revise everything you enter here.
Step 3: Before finishing this form, you should make sure that form fields are filled in as intended. Once you believe it is all good, click on “Done." Join us now and instantly get access to direct deposit 160, set for download. Each and every change made is conveniently kept , allowing you to change the file later on when required. FormsPal offers protected document tools devoid of data record-keeping or sharing. Be assured that your details are safe with us!