
Complete the Biomet 3i complaint form online using the FormsPal® PDF tool. No software download is required. Follow these steps to fill out the 3I Biomet form accurately:
Step 1: Click the "Get Form" button above. It will open the PDF editor so you can begin filling in your form.
Step 2: The PDF editor lets you do more than fill blank fields. Add customized text, adjust original content, insert graphics, and sign the document when ready.
This document requires specific information, so take time to enter each field correctly.
1. Fill out the biomet 3i complaint form with all required fields. Review the entire form before moving to the next section.
2. Complete the following fields: Warranty Form To comply with, NonIntegration Loss of, If this event involved an implant, M Rev, and Restored.
Double-check the implant event fields before continuing - errors in this section can delay the warranty claim.
3. This section covers patient-specific implant conditions: For Implants only - Did the patient, Smoker, Osteoporosis, Diabetes, Other, Yes, No, High density Type I, Xenograft Alloplast, Hybrid, Single Stage transgingival Two, No Yes describe material below, Autogenous Allograft, and Moderate density Type II Low. Fill in every field that applies.
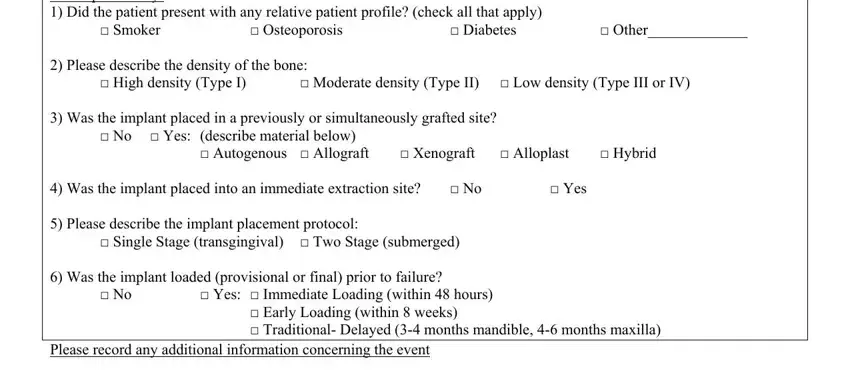
4. Complete the final section: Please describe the density of, Date, Send To, BIOMET i, Regulatory ServicesImplant Warranty, Riverside Drive, Palm Beach Gardens FL, and Phone Fax. These fields identify the submission address and contact information for Biomet 3I's Regulatory Services team.
Step 3: After completing all fields, click "Done" to save and download your form. Create a FormsPal account to access the biomet 3i complaint form at any time. All changes are saved automatically.
Common Questions About the 3I Form Biomet
What is the 3I Form Biomet used for?
The 3I Form Biomet is the official Biomet 3I dental implant warranty and complaint form. Dental professionals use it to report adverse events under FDA Medical Device Reporting (MDR) rules and to request a warranty replacement for a failed implant. It is submitted to Biomet 3I's Regulatory Services along with the returned device when available.
Who should complete the Biomet 3i warranty form?
Any dental practitioner, oral surgeon, or clinic that placed a Biomet 3I implant and observed a non-integration event, implant failure, or device malfunction must complete this form. Related documentation includes the ADA dental claim form and, for follow-up care, a dental treatment consent form.
Is the 3I Biomet form available online?
Yes. FormsPal provides a free online PDF editor to fill out the 3I Biomet form directly in your browser. Once complete, download the signed PDF and mail it to Biomet 3I's Regulatory Services department in Palm Beach Gardens, FL.