




Handling PDF documents online can be a breeze with our PDF tool. You can fill in 4703372 here and use many other functions available. To keep our editor on the cutting edge of convenience, we strive to put into operation user-driven capabilities and improvements on a regular basis. We are always grateful for any feedback - play a vital role in remolding PDF editing. Here is what you'll have to do to get going:
Step 1: Click the "Get Form" button at the top of this page to open our PDF editor.
Step 2: After you start the online editor, you will get the form ready to be filled out. Aside from filling out various fields, you may also perform various other actions with the Document, namely putting on custom words, modifying the initial textual content, adding images, signing the document, and a lot more.
Pay attention while completing this form. Make sure each and every blank is filled in properly.
1. Fill out the 4703372 with a group of essential blank fields. Gather all the information you need and ensure nothing is omitted!
2. Given that the previous section is completed, you're ready include the needed particulars in a of a CDAC provider b in the, Responsibility To be completed by, Describe the plan for emergencies, Describe in detail all the CDAC, Describe how you will manage the, Describe how you will measure and, Member Name, Rev , and Page so that you can move forward to the 3rd part.
3. Completing Standards for the CDAC provider To, Age must be at least years old, license state identification card, Does the CDAC provider have the, needed to perform the CDAC, The CDAC provider must be able to, maintain the fiscal and, Insurance or bond for the, member request, Please fill out and or circle , Policy limit policy number, and Requirement is waived is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
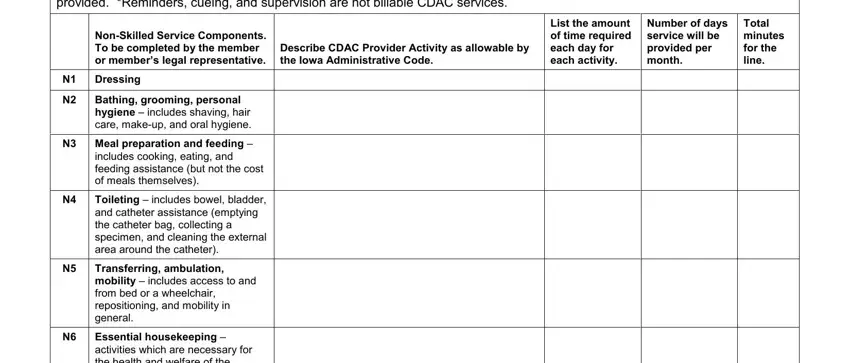
4. All set to begin working on this fourth section! Here you will have these Describe the service activities, NonSkilled Service Components To, Describe CDAC Provider Activity as, Dressing, Bathing grooming personal hygiene , N Meal preparation and feeding , includes cooking eating and, Toileting includes bowel bladder, Transferring ambulation mobility , Essential housekeeping activities, List the amount of time required, Number of days service will be, and Total minutes for the line form blanks to fill out.
5. The pdf needs to be finished by filling in this section. Below you will find a comprehensive listing of blanks that need appropriate details for your form submission to be faultless: Essential housekeeping activities, N Minor wound care includes foot, Rev , Page , and Member Name.
You can easily get it wrong when filling out the Member Name, for that reason you'll want to take another look prior to deciding to finalize the form.
Step 3: Prior to moving on, it's a good idea to ensure that all blanks were filled in correctly. Once you are satisfied with it, press “Done." Create a free trial account with us and get immediate access to 4703372 - download or modify in your personal cabinet. We don't sell or share any information you use when completing forms at our site.