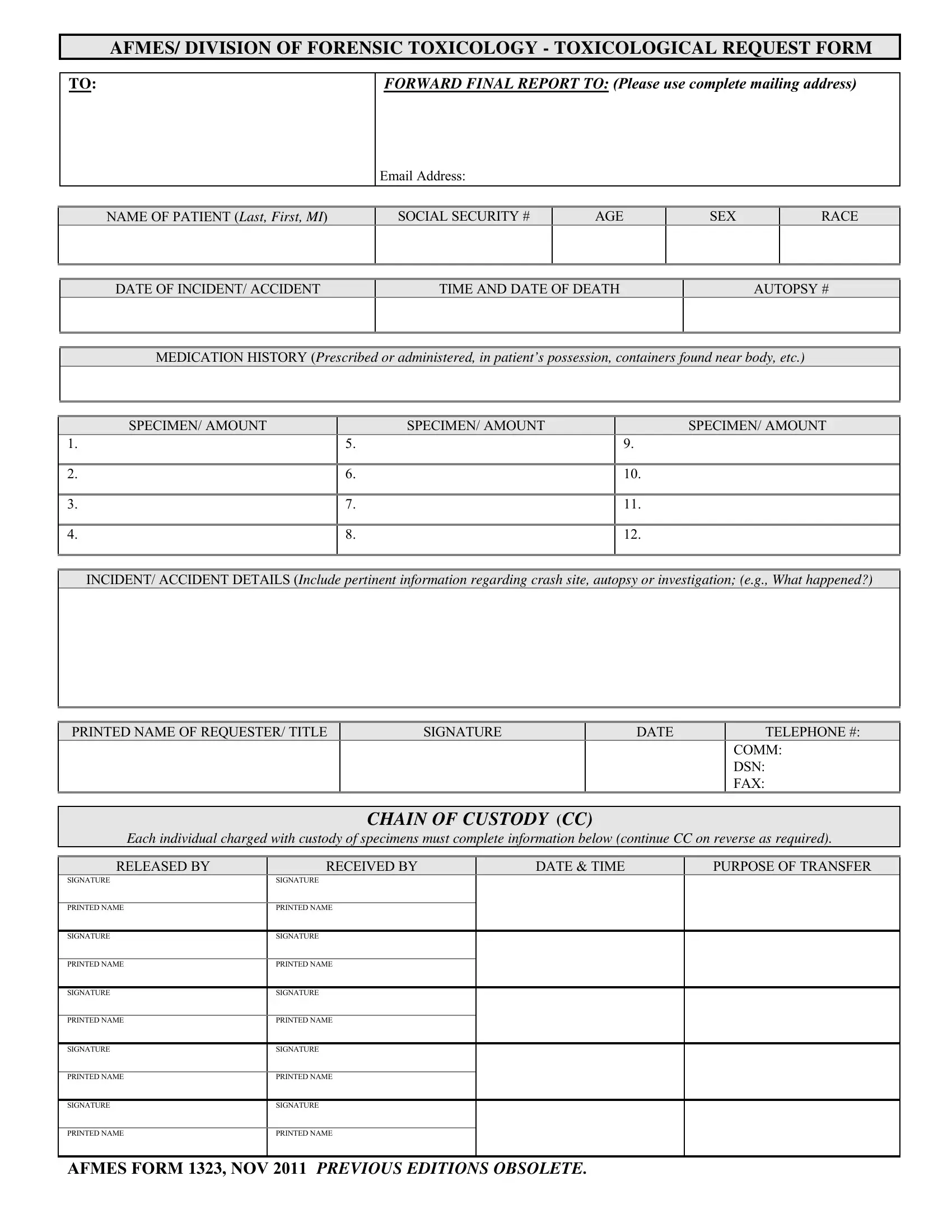
In the realm of forensic toxicology, the AFMES 1323 form plays a pivotal role, serving as the primary means of requesting toxicological analysis in situations where understanding the chemical substances present in a body is crucial. This form, issued by the Armed Forces Medical Examiner System's Division of Forensic Toxicology, is meticulously designed to gather comprehensive information that includes the patient's identification details, such as name, social security number, age, sex, and race, as well as specifics related to the incident or accident leading to the need for analysis. The date and time of both the incident and the patient's death, alongside a detailed medication history, are critical for the analysis process. Moreover, the form provides a structured way to list specimens collected for toxicology testing, ensuring clarity regarding the types and amounts of samples submitted. Detailed incident or accident information offers contextual insights that can be vital for the interpretation of toxicological results. The form further facilitates a clear chain of custody for the specimens, highlighting the importance of maintaining integrity and accountability from collection to analysis. By requiring information such as the names and signatures of individuals transferring the specimens, along with the purpose of each transfer, the form safeguards the authenticity and reliability of the samples, an aspect that is paramount in forensic investigations. Ultimately, the AFMES 1323 form is essential for ensuring that the pertinent questions surrounding an incident or accident can be answered with the highest degree of precision and reliability.
| Question | Answer |
|---|---|
| Form Name | Afmes Form 1323 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | afmes, TOXICOLOGICAL, afmes form 18 fillable pdf, EDITIONS |
AFMES/ DIVISION OF FORENSIC TOXICOLOGY - TOXICOLOGICAL REQUEST FORM
TO:
FORWARD FINAL REPORT TO: (Please use complete mailing address)
EMAIL ADDRESS:
NAME OF PATIENT (Last, First, MI)
SOCIAL SECURITY #
AGE
SEX
RACE
DATE OF INCIDENT/ ACCIDENT
TIME AND DATE OF DEATH
AUTOPSY #
MEDICATION HISTORY (Prescribed or administered, in patient’s possession, containers found near body, etc.)
SPECIMEN/ AMOUNT |
SPECIMEN/ AMOUNT |
SPECIMEN/ AMOUNT |
1. |
5. |
9. |
|
|
|
2. |
6. |
10. |
|
|
|
3. |
7. |
11. |
|
|
|
4. |
8. |
12. |
|
|
|
INCIDENT/ ACCIDENT DETAILS (Include pertinent information regarding crash site, autopsy or investigation; (e.g., What happened?)
PRINTED NAME OF REQUESTER/ TITLE |
SIGNATURE |
DATE |
TELEPHONE #: |
|
|
|
|
COMM: ( |
) |
|
|
|
DSN: |
|
|
|
|
FAX: |
|
CHAIN OF CUSTODY (CC)
Each individual charged with custody of specimens must complete information below (continue CC on reverse as required).
RELEASED BY |
RECEIVED BY |
DATE & TIME |
PURPOSE OF TRANSFER |
SIGNATURE
SIGNATURE
PRINTED NAME
PRINTED NAME
SIGNATURE
SIGNATURE
PRINTED NAME
PRINTED NAME
SIGNATURE
SIGNATURE
PRINTED NAME
PRINTED NAME
SIGNATURE
SIGNATURE
PRINTED NAME
PRINTED NAME
SIGNATURE
SIGNATURE
PRINTED NAME
PRINTED NAME
AFMES FORM 1323, NOV 2011 PREVIOUS EDITIONS OBSOLETE.