Navigating the requirements for commercial pesticide applicators in Washington can feel complex, but the Agr 702 4279 form stands as a crucial piece in ensuring these professionals meet the state's financial responsibility standards. Required by the Washington State Department of Agriculture Pesticide Management Division, this Financial Responsibility Insurance Certificate (FRIC) is a testament to the commitment of commercial applicators in upholding financial coverage for potential damages that could arise from their pesticide application activities. Unlike a general insurance policy, this certificate specifically caters to the bodily injury and property damage tied to pesticide use, setting a clear boundary with a minimum liability coverage and addressing exclusions comprehensively. Tailored not just for new licensees but also for existing ones needing to renew their insurance coverage, the form serves as a bridge between commercial applicators, their insurance agents, and regulatory oversight. It's a safeguard for both the applicators and the community, ensuring that there is a financial safety net in place for the unintended consequences of pesticide application. Furthermore, it distinguishes between general pesticide application and wood destroying organism (WDO) inspections, highlighting the unique requirements for those engaging in complete WDO inspections during property transactions. With detailed instructions on its completion and submission, the Agr 702 4279 form epitomizes an essential step towards compliance and protection in the pesticide application industry in Washington.
| Question | Answer |
|---|---|
| Form Name | Agr Form 702 4279 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | syngenta principal certificate, principal certificate, pesticides principal certificate, principal certificate for seeds |
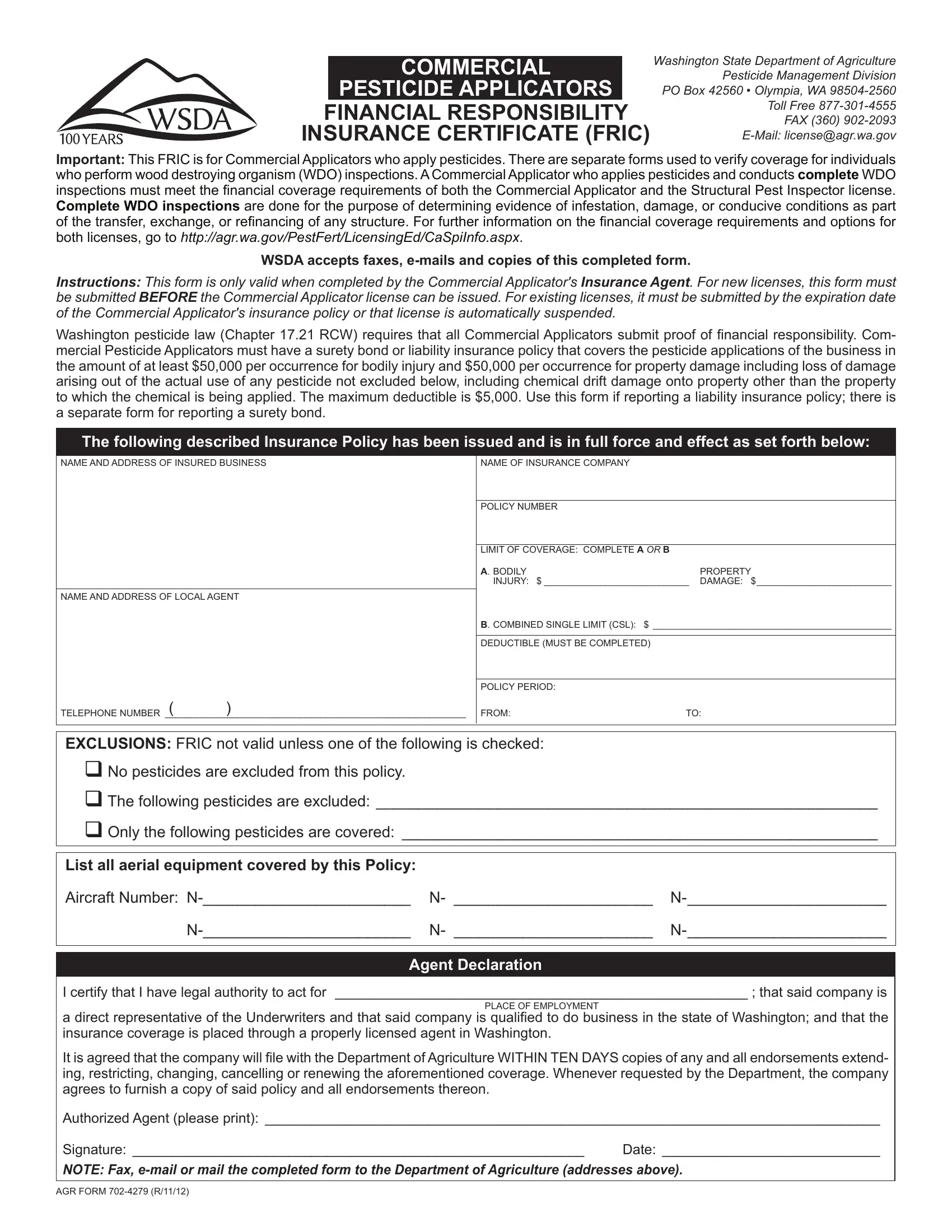
COMMERCIAL
PESTICIDE APPLICATORS
FINANCIAL RESPONSIBILITY
INSURANCE CERTIFICATE (FRIC)
Washington State Department of Agriculture Pesticide Management Division PO Box 42560 • Olympia, WA
Important: This FRIC is for Commercial Applicators who apply pesticides. There are separate forms used to verify coverage for individuals
who perform wood destroying organism (WDO) inspections. A Commercial Applicator who applies pesticides and conducts complete WDO inspections must meet the inancial coverage requirements of both the Commercial Applicator and the Structural Pest Inspector license.
Complete WDO inspections are done for the purpose of determining evidence of infestation, damage, or conducive conditions as part of the transfer, exchange, or reinancing of any structure. For further information on the inancial coverage requirements and options for
both licenses, go to http://agr.wa.gov/PestFert/LicensingEd/CaSpiInfo.aspx.
WSDA accepts faxes,
Instructions: This form is only valid when completed by the Commercial Applicator's Insurance Agent. For new licenses, this form must be submitted BEFORE the Commercial Applicator license can be issued. For existing licenses, it must be submitted by the expiration date of the Commercial Applicator's insurance policy or that license is automatically suspended.
Washington pesticide law (Chapter 17.21 RCW) requires that all Commercial Applicators submit proof of inancial responsibility. Com- mercial Pesticide Applicators must have a surety bond or liability insurance policy that covers the pesticide applications of the business in the amount of at least $50,000 per occurrence for bodily injury and $50,000 per occurrence for property damage including loss of damage arising out of the actual use of any pesticide not excluded below, including chemical drift damage onto property other than the property to which the chemical is being applied. The maximum deductible is $5,000. Use this form if reporting a liability insurance policy; there is a separate form for reporting a surety bond.
The following described Insurance Policy has been issued and is in full force and effect as set forth below:
NAME AND ADDRESS OF INSURED bUSINESS
NAME AND ADDRESS OF LOCAL AGENT
TELEPHONE NUMbER __________________________________________________________( )
NAME OF INSURANCE COMPANY
POLICY NUMbER
LIMIT OF COVERAGE: COMPLETE A Or B |
|
A. bODILY |
PROPERTY |
INjURY: $ ____________________________ |
DAMAGE: $__________________________ |
B. COMbINED SINGLE LIMIT (CSL): $ ______________________________________________
DEDUCTIbLE (MUST bE COMPLETED)
POLICY PERIOD:
FROM:TO:
EXCLUSIONS: FRIC not valid unless one of the following is checked:
No pesticides are excluded from this policy.
The following pesticides are excluded: __________________________________________________________
Only the following pesticides are covered: _______________________________________________________
List all aerial equipment covered by this Policy: |
|
|
Aircraft Number: |
N- _______________________ |
|
N- _______________________ |
||
|
|
|
Agent Declaration
I certify that I have legal authority to act for _____________________________________________________ ; that said company is
PLACE OF EMPLOYMENT
a direct representative of the Underwriters and that said company is qualiied to do business in the state of Washington; and that the
insurance coverage is placed through a properly licensed agent in Washington.
It is agreed that the company will ile with the Department of Agriculture WITHIN TEN DAYS copies of any and all endorsements extend- ing, restricting, changing, cancelling or renewing the aforementioned coverage. Whenever requested by the Department, the company
agrees to furnish a copy of said policy and all endorsements thereon.
Authorized Agent (please print): _______________________________________________________________________________
Signature: __________________________________________________________ |
Date: ____________________________ |
NOTE: Fax,
AGR FORM