
Handling PDF documents online is super easy using our PDF editor. Anyone can fill in youth flight registration here in a matter of minutes. Our professional team is constantly endeavoring to develop the editor and enable it to be much faster for users with its extensive features. Enjoy an ever-evolving experience today! Starting is easy! All you should do is take the next easy steps directly below:
Step 1: Open the PDF doc in our tool by clicking the "Get Form Button" in the top section of this webpage.
Step 2: As soon as you open the PDF editor, you will find the document prepared to be filled out. Other than filling out various blanks, you might also do many other actions with the Document, namely putting on custom textual content, changing the original text, inserting illustrations or photos, signing the PDF, and more.
This form will need particular data to be typed in, thus be sure you take your time to enter what's expected:
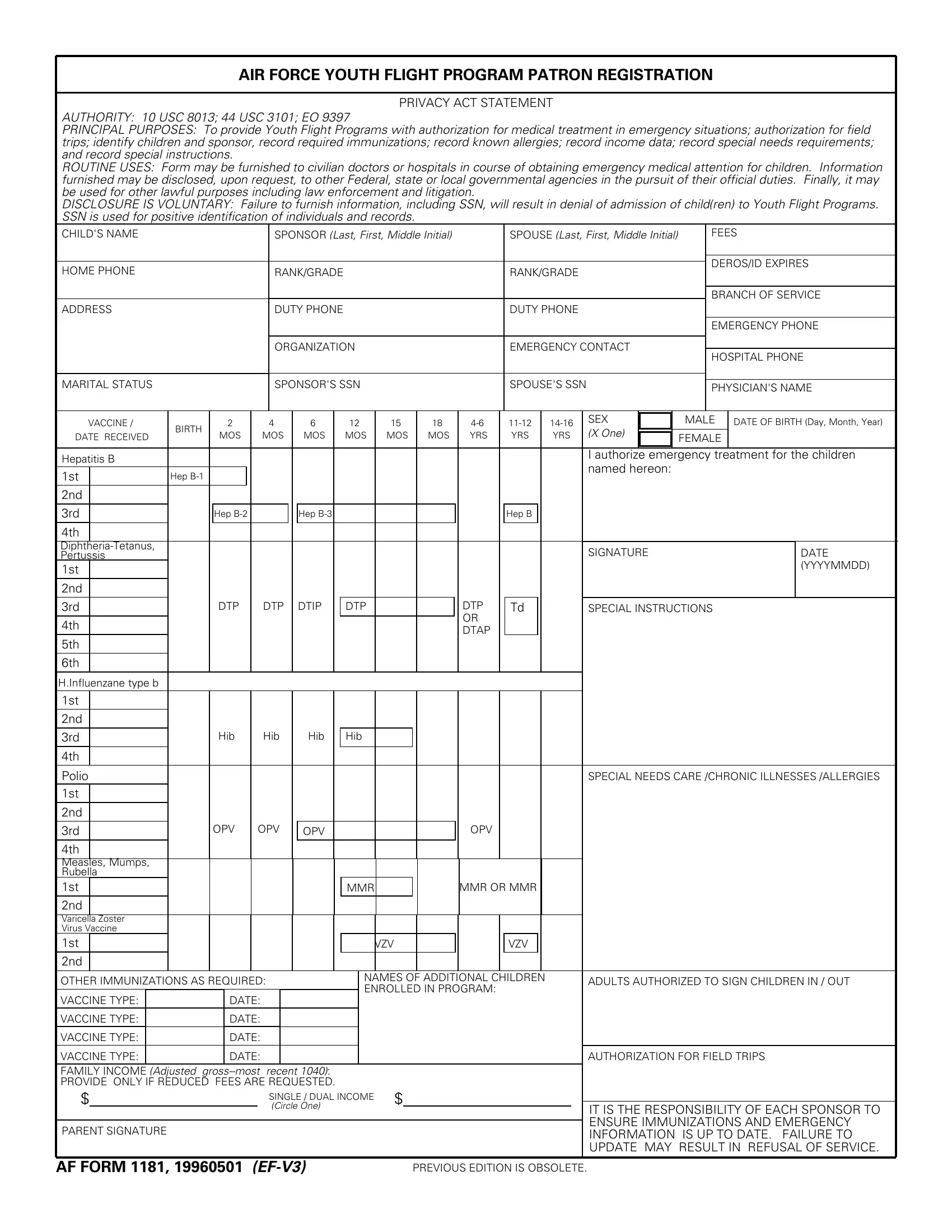
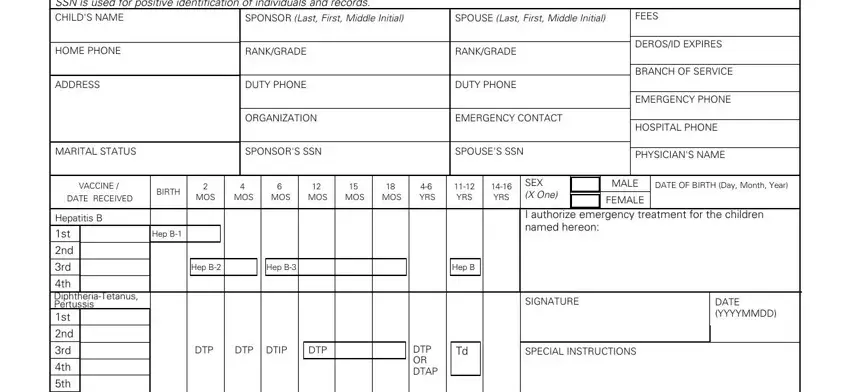
1. The youth flight registration requires particular details to be entered. Be sure that the next blanks are completed:
2. Once your current task is complete, take the next step – fill out all of these fields - Polio, th Measles Mumps Rubella st, nd Varicella Zoster Virus Vaccine, SPECIAL NEEDS CARE CHRONIC, OPV, OPV, OPV, OPV, MMR, MMR OR MMR, VZV, VZV, OTHER IMMUNIZATIONS AS REQUIRED, NAMES OF ADDITIONAL CHILDREN, and ADULTS AUTHORIZED TO SIGN CHILDREN with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
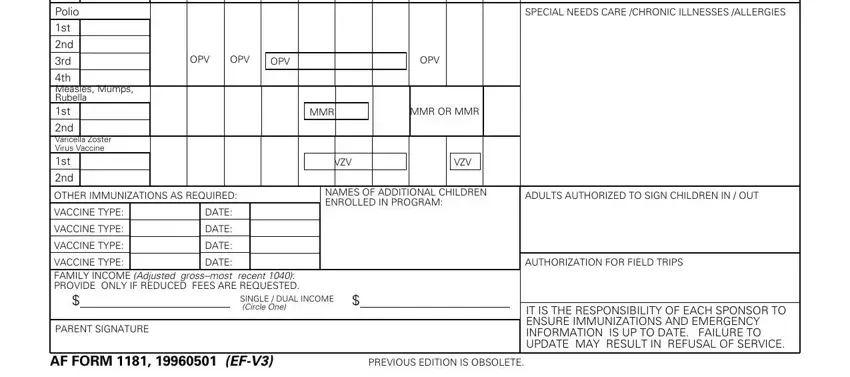
Always be very mindful while completing VZV and OTHER IMMUNIZATIONS AS REQUIRED, since this is where a lot of people make some mistakes.
Step 3: Before obtaining the next step, check that form fields were filled in the proper way. The moment you’re satisfied with it, click “Done." Go for a 7-day free trial account at FormsPal and obtain immediate access to youth flight registration - which you may then use as you want in your personal account. Here at FormsPal.com, we do our utmost to make sure your information is maintained private.