When individuals encounter the necessity to dispute a decision regarding their insurance claim with American Heritage Life Insurance Company, an Allstate Appeal form becomes an indispensable tool. Distributed under the umbrella of Allstate Workplace Division, this form facilitates a structured pathway for policyholders to appeal against determinations made on their claims, encompassing various insurance coverages like Wellness Screening, Intensive Care, Waiver of Premium, Heart/Stroke, and Cancer/Specified Disease. Not to be misconstrued as an admission of liability or a waiver of any insurance contract conditions, the form stipulates clear instructions for completion to avoid delays in the appeal process. Important features include a provision for attaching itemized bills, notifying of a return to work, and specifying any periods of disability or confinement. Furthermore, it emphasizes compliance with federal laws regarding social security number verification and backup withholding requirements. Significantly, the form also integrates a fraud warning, tailored to the legal stipulations of different states, aiming to deter the submission of false, incomplete, or misleading information. This multi-faceted document underscores the intricate balance between providing policyholders a means to seek redress and ensuring the integrity of the claims process.
| Question | Answer |
|---|---|
| Form Name | Allstate Appeal Printable Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | Allstate, obstetrical, Claimant, designee |
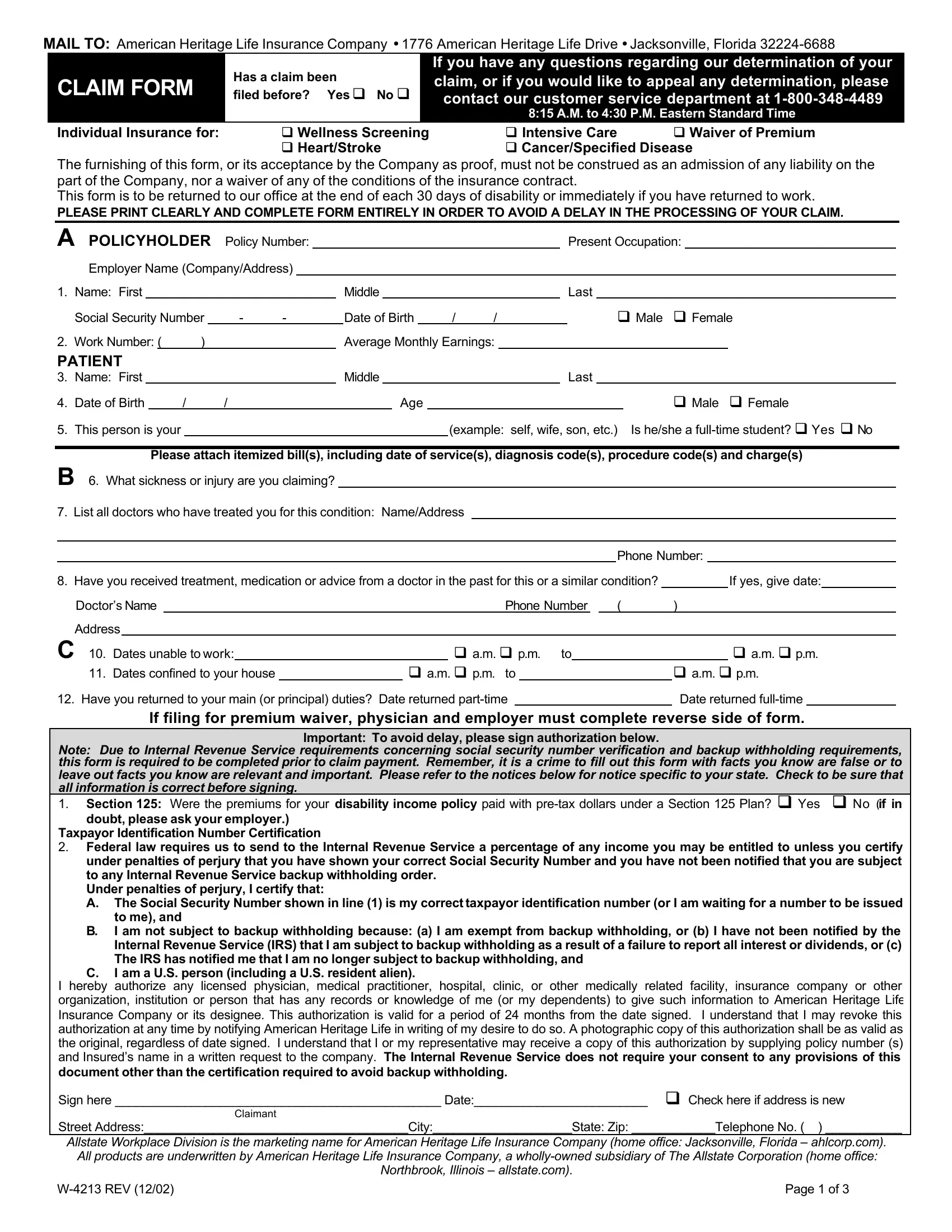
MAIL TO: American Heritage Life Insurance Company ∙ 1776 American Heritage Life Drive ∙ Jacksonville, Florida
CLAIM FORM
Has a claim been
filed before? Yes q No q
If you have any questions regarding our determination of your claim, or if you would like to appeal any determination, please contact our customer service department at
8:15 A.M. to 4:30 P.M. Eastern Standard Time
Individual Insurance for: |
q Wellness Screening |
q Intensive Care |
q Waiver of Premium |
|
q Heart/Stroke |
q Cancer/Specified Disease |
|
The furnishing of this form, or its acceptance by the Company as proof, must not be construed as an admission of any liability on the part of the Company, nor a waiver of any of the conditions of the insurance contract.
This form is to be returned to our office at the end of each 30 days of disability or immediately if you have returned to work.
PLEASE PRINT CLEARLY AND COMPLETE FORM ENTIRELY IN ORDER TO AVOID A DELAY IN THE PROCESSING OF YOUR CLAIM.
A POLICYHOLDER |
Policy Number: |
|
|
|
|
|
|
|
|
|
|
|
|
Present Occupation: |
|||||||||||||
|
Employer Name (Company/Address) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
1. |
Name: First |
|
|
|
|
|
|
|
|
|
Middle |
|
|
|
|
|
|
|
Last |
|
|||||||
|
Social Security Number |
|
- |
- |
|
|
|
Date of Birth |
|
/ |
/ |
|
|
|
|
q Male q Female |
|||||||||||
2. |
Work Number: ( |
) |
|
|
|
|
|
|
Average Monthly Earnings: |
|
|
|
|
|
|
|
|||||||||||
PATIENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
3. |
Name: First |
|
|
|
|
|
|
|
|
|
Middle |
|
|
|
|
|
|
|
Last |
|
|||||||
4. |
Date of Birth |
|
/ |
|
/ |
|
|
|
|
|
|
Age |
|
|
|
|
|
|
|
|
q Male q Female |
||||||
5. |
This person is your |
|
|
|
|
|
|
|
|
|
|
|
|
|
(example: |
self, wife, son, etc.) Is he/she a |
|||||||||||
Please attach itemized bill(s), including date of service(s), diagnosis code(s), procedure code(s) and charge(s)
B6. What sickness or injury are you claiming?
7. List all doctors who have treated you for this condition: Name/Address
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone Number: |
|
|||||
8. Have you received treatment, medication or advice from a doctor in the past for this or a similar condition? |
|
|
|
If yes, give date: |
||||||||||||||||
Doctor’s Name |
|
|
|
Phone Number |
|
|
( |
) |
|
|
|
|
||||||||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
C 10. |
Dates unable to work: |
|
|
|
q a.m. q p.m. to |
|
|
|
|
q a.m. q p.m. |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
11. |
Dates confined to your house |
|
|
q a.m. q p.m. to |
|
|
|
q a.m. q p.m. |
||||||||||||
12. Have you returned to your main (or principal) duties? |
Date returned |
|
|
|
Date returned |
|
||||||||||||||
If filing for premium waiver, physician and employer must complete reverse side of form.
Important: To avoid delay, please sign authorization below.
Note: Due to Internal Revenue Service requirements concerning social security number verification and backup withholding requirements, this form is required to be completed prior to claim payment. Remember, it is a crime to fill out this form with facts you know are false or to
leave out facts you know are relevant and important. Please refer to the notices below for notice specific to your state. Check to be sure that all information is correct before signing.
1. Section 125: Were the premiums for your disability income policy paid with
doubt, please ask your employer.) Taxpayor Identification Number Certification
2.Federal law requires us to send to the Internal Revenue Service a percentage of any income you may be entitled to unless you certify under penalties of perjury that you have shown your correct Social Security Number and you have not been notified that you are subject to any Internal Revenue Service backup withholding order.
Under penalties of perjury, I certify that:
A.The Social Security Number shown in line (1) is my correct taxpayor identification number (or I am waiting for a number to be issued to me), and
B.I am not subject to backup withholding because: (a) I am exempt from backup withholding, or (b) I have not been notified by the Internal Revenue Service (IRS) that I am subject to backup withholding as a result of a failure to report all interest or dividends, or (c) The IRS has notified me that I am no longer subject to backup withholding, and
C.I am a U.S. person (including a U.S. resident alien).
I hereby authorize any licensed physician, medical practitioner, hospital, clinic, or other medically related facility, insurance company or other organization, institution or person that has any records or knowledge of me (or my dependents) to give such information to American Heritage Life Insurance Company or its designee. This authorization is valid for a period of 24 months from the date signed. I understand that I may revoke this authorization at any time by notifying American Heritage Life in writing of my desire to do so. A photographic copy of this authorization shall be as valid as the original, regardless of date signed. I understand that I or my representative may receive a copy of this authorization by supplying policy number (s) and Insured’s name in a written request to the company. The Internal Revenue Service does not require your consent to any provisions of this document other than the certification required to avoid backup withholding.
Sign here _______________________________________________ Date:_________________________ q Check here if address is new
Claimant
Street Address:______________________________________City:____________________State: Zip: ____________Telephone No. ( ) ___________
Allstate Workplace Division is the marketing name for American Heritage Life Insurance Company (home office: Jacksonville, Florida – ahlcorp.com). All products are underwritten by American Heritage Life Insurance Company, a
Northbrook, Illinois – allstate.com).
Page 1 of 3 |
ATTENDING PHYSICIAN’S STATEMENT
|
Individual Insurance for: |
q Wellness Screening |
q Intensive Care |
|
q Waiver of Premium |
|||||
|
|
|
q Heart/Stroke |
q Cancer/Specified Disease |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
D Patient’s Name |
|
|
|
|
|
|
Age |
||
|
|
|
|
|
|
|
|
|
||
1. |
Diagnosis: (Describe complications if any) Is condition due to pregnancy? |
q Yes |
q No |
|
|
|||||
|
|
|
|
|
|
|
||||
|
|
If “yes”, what was approximate date of commencement of pregnancy? |
Date – MO/DAY/YR |
|
|
|||||
2. |
When did symptoms first appear or accident happen? |
|
Date – MO/DAY/YR |
|
|
|||||
3. |
When did patient first consult you for this condition? |
|
Date – MO/DAY/YR |
|
|
|||||
4. |
Has patient ever had same or similar condition? (If “yes”, state when and describe) |
q Yes q No |
|
|
||||||
5.Describe any other diseases or infirmity affecting present condition.
6.Nature of surgical or obstetrical procedure, if any (describe fully).
Charge for this procedure and where performed? |
$ |
|
|
|
Date – MO/DAY/YR |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
If in hospital, |
q in patient |
|
q outpatient |
|||||
7. |
Please attach itemized bill(s), date(s) of service, procedure code(s) and charge(s). |
|
|
|
|
|
|
|
||||||||||
8. |
Is patient still under your care for this condition? |
|
|
|
q Yes |
q No |
|
|
|
|
|
|
|
|||||
|
If discharged give date |
|
|
|
|
|
Date – MO/DAY/YR. |
|
|
|
|
|||||||
9. |
If patient is/was hospitalized, give name and address of hospital. |
|
|
|
|
|
|
|
|
|
||||||||
|
Hospital |
|
|
City |
|
|
|
|
|
State |
|
|
|
|||||
|
Date admitted – MO/DAY/YR |
|
Date discharged – MO/DAY/YR |
|
|
|
|
|
|
|
|
|||||||
10. How long was or will patient be continuously totally disabled (unable to work)? From Date – MO/DAY/YR |
|
|
through |
|
||||||||||||||
11.If still disabled, when do you expect patient to resume full duties?
12.Name and address of referring physician if any
Name |
|
Address |
|
|
|
||
City |
|
|
State |
|
|
Zip |
|
PHYSICIAN VERIFICATION
Signed |
|
, MD |
Date – MO/DAY/YR |
|
|
Phone ( |
) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
City/Town |
|
|
|
|
|
|
|||
State/Province |
|
|
Zip Code |
|
|
|
|
|
|
|||
Remember, it is a crime to fill out this form with facts you know are false or to leave out facts you know are relevant and important. Please refer to page 3 for notice specific to your state. Check to be sure that all information is correct before signing.
EEMPLOYER’S STATEMENT
1. |
I hereby certify that |
|
did not perform any part of his/her work from, |
|
|||||
|
to, |
|
|
|
|
|
|
||
2. |
When recovered, will he/she resume work? |
|
|
If not why? |
|
||||
Remarks
Name of Employer |
|
|
|
Date |
|
Address |
|
|
||
By |
|
|
Official Position |
|
|
Telephone number ( |
) |
|||
|
|
|
|
|
|
|
|
|
|
|
Allstate Workplace Division is the marketing name for American Heritage Life Insurance Company (home office: Jacksonville, Florida – ahlcorp.com). All products are underwritten by American Heritage Life Insurance Company, a
Northbrook, Illinois – allstate.com).
Page 2 of 3 |

NOTICE IN ALASKA, ARKANSAS, KENTUCKY, LOUISIANA, MAINE, NEW JERSEY, NEW MEXICO, AND VIRGINIA: Any person who knowingly and with intent to injure, defraud or deceive an insurance company files a claim containing false, incomplete or misleading information may be prosecuted under state law.
NOTICE IN DELAWARE, IDAHO, INDIANA, MINNESOTA, NEW HAMPSHIRE, AND OKLAHOMA: Any person who knowingly and with intent to injure, defraud or deceive an insurance company files a claim containing false, incomplete or misleading information is guilty of a felony.
NOTICE IN ARIZONA: For your protection Arizona law requires the following statement to appear on this form. Any person who knowingly presents a false or fraudulent claim for payment of loss is subject to criminal and civil penalties.
NOTICE IN CALIFORNIA: For your protection, California law requires the following to appear on this form. Any person who knowingly presents false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.
NOTICE IN COLORADO: It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado division of insurance within the department of regulatory agencies.
NOTICE IN FLORIDA: Any person who knowingly and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application containing any false, incomplete, or misleading information is guilty of a felony of the third degree.
NOTICE IN OHIO: Any person who, with intent to defraud or knowing that he is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud.
NOTICE IN PENNSYLVANIA: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
NOTICE IN DISTRICT OF COLUMBIA: WARNING: It is a crime to provide false or misleading information to an insurer for the purpose of defrauding the insurer or any other person. Penalties include imprisonment and/or fines. In addition, an insurer may deny insurance benefits if false information materially related to a claim was provided by the applicant.
NOTICE IN TENNESSEE: It is a crime to knowingly provide false, incomplete or misleading information to an insurance company for the purpose of defrauding the company. Penalties include imprisonment, fines and denial of insurance benefits.
NOTICE IN TEXAS: Any person who knowingly presents a false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.
Allstate Workplace Division is the marketing name for American Heritage Life Insurance Company (home office: Jacksonville, Florida – ahlcorp.com). All products are underwritten by American Heritage Life Insurance Company, a
Northbrook, Illinois – allstate.com).
Page 3 of 3 |