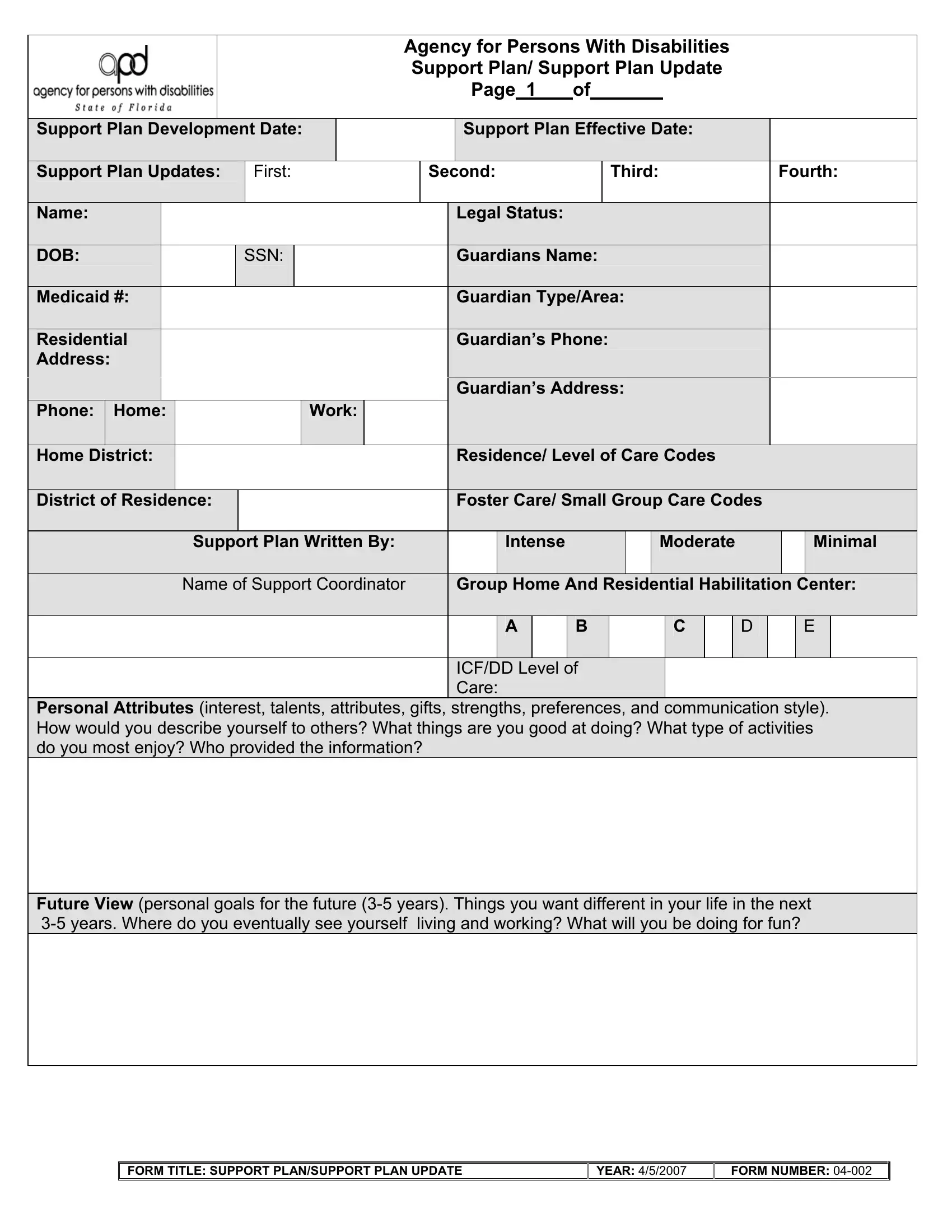
The Agency for Persons With Disabilities Support Plan, also known as the Support Plan Update form, is a crucial document aimed at identifying and outlining the necessary supports and services for individuals with disabilities to lead a quality life tailored to their unique needs, preferences, and goals. The form, designated with the form number 04-002 and last updated on April 5, 2007, acts as a comprehensive planning tool that covers a wide array of critical aspects concerning the individual's care and future planning. It details personal attributes including interests, talents, and communication styles, which helps in painting a clear picture of the individual's identity and aspirations. Furthermore, it addresses the individual's current and future living situations, health concerns, including a detailed medication list, and assistive devices used, ensuring all aspects of their well-being are considered. Additionally, it lays out the individual's goals for the upcoming year, the support and services needed to achieve these goals, as well as routine services essential for maintaining health and safety. With sections for individual and guardian consent, the form underscores the importance of the individual's active participation in the development of their support plan, highlighting their rights and the collaborative nature of the planning process. This document serves not only as a plan but also as a commitment from multiple parties to work together towards achieving the best possible outcomes for the individual.
| Question | Answer |
|---|---|
| Form Name | Apd Support Plan Form |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | updated support plan apd, apd support plan update, apd printable person centered support plan, what is a sample support plan for apd |
|
|
|
|
|
|
|
|
|
|
Agency for Persons With Disabilities |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
Support Plan/ Support Plan Update |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 1 |
of___ |
__ |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Support Plan Development Date: |
|
|
|
|
|
Support Plan Effective Date: |
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Support Plan Updates: |
|
First: |
|
Second: |
|
|
Third: |
|
|
Fourth: |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
Legal Status: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DOB: |
|
|
SSN: |
|
|
|
|
|
|
Guardians Name: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medicaid #: |
|
|
|
|
|
|
|
|
|
|
|
Guardian Type/Area: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Residential |
|
|
|
|
|
|
|
|
|
|
|
Guardian’s Phone: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Guardian’s Address: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Phone: |
Home: |
|
|
|
|
Work: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home District: |
|
|
|
|
|
|
|
|
|
|
Residence/ Level of Care Codes |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
District of Residence: |
|
|
|
|
|
|
|
|
|
Foster Care/ Small Group Care Codes |
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Support Plan Written By: |
|
|
|
|
Intense |
|
|
|
|
Moderate |
|
|
|
|
|
Minimal |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Support Coordinator |
|
|
|
Group Home And Residential Habilitation Center: |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
B |
|
|
|
|
C |
|
|
D |
|
|
|
E |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ICF/DD Level of |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Care: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Personal Attributes (interest, talents, attributes, gifts, strengths, preferences, and communication style). How would you describe yourself to others? What things are you good at doing? What type of activities do you most enjoy? Who provided the information?
Future View (personal goals for the future
FORM TITLE: SUPPORT PLAN/SUPPORT PLAN UPDATE |
YEAR: 4/5/2007 |
FORM NUMBER:
Agency for Persons With Disabilities
Support Plan/ Support Plan Update Page of
Name:
Support Plan Effective Date:
Life Area
Present situation (in the life areas of home, daily activities/work/school and personal/social).
Include a brief functional description of : (1) capabilities, (2) daily activities,
(3) interactions with others, (4) valued roles, (5) community opportunities,
(6)supports and services currently being received (both paid and unpaid), (7) issues or concerns (health, challenging behaviors or situations) the person is experiencing,
(8)any changes the person wants in their present situation, and (9) important relationships in the person’s life. Also include a brief summary of personal goals achieved in the past year and/or the status toward completion. (Add additional pages if needed). This summary will serve as the annual report.
FORM TITLE: SUPPORT PLAN/SUPPORT PLAN UPDATE |
YEAR: 4/5/2007 |
FORM NUMBER:
Agency for Persons With Disabilities
Support Plan/ Support Plan Update Page of
Name:
Support Plan Effective
Date:
Health Summary: Describe any health concerns and how it impacts on the person. What health concerns do you have? Describe the preventative health services that are needed to stay healthy.
( Attach additional pages and/or reports if needed.)
Who helps you manage |
|
|
|
Relationship: |
|
Phone: |
|
|||
your health care? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Assistive or Adaptive Equipment: |
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Identify glasses, dentures, equipment, etc. What adaptive equipment do you use and what is it used for?
Medications: |
|
Yes, list below |
|
No |
|
Identify all meds: The name and dosage schedule, purpose and any problems/side effects being experienced. Any r problems, e.g., drowsiness, rashes, etc?
Current as of:
Medication Name Dosage and schedule Purpose or Diagnosis Problems/ Side Effects Noted
Note: Pages A, B, and C should be completed by the Support Coordinator Prior to the Support Plan Meeting.
FORM TITLE: SUPPORT PLAN/SUPPORT PLAN UPDATE |
YEAR: 4/5/2007 |
FORM NUMBER:
Agency for Persons With Disabilities Support Plan/ Support Plan Update- Page of
Name:
Support Plan Effective
Date:
Personal Goals for Upcoming Year: What do you want to accomplish this year? What are the most important things you want to see happen in your life?
*Support/Services Needed: Include all natural, generic, community and paid supports. Identify the type of service and who is responsible. (include only those services needed to accomplish personal goals.)
Other supports/Services Needed: Routine services that are not specifically related to the accomplishment of personal goals but are essential supports/services needed to ensure that the person’s health and safety are maintained.
Who will take the Lead? Identify the person who will take the lead on scheduling appointments or other type of actions needed.
NOTE: Support coordinator has overall responsibility to coordinate the provision of all supports and services. Support coordinator is identified as responsible in situations in which the coordinator has a definite role/ specific task the coordinator is responsible for completing.
FORM TITLE: SUPPORT PLAN/SUPPORT PLAN UPDATE |
YEAR: 4/5/2007 |
FORM NUMBER:

Agency for Persons With Disabilities Support Plan/ Support Plan Update- Page of
Name:
Support Plan Effective
Date:
Individual/Guardian Consent: I have participated in the development of the plan and I agree to the contents. I have been informed of my due process rights under Florida Statutes 120 and that I may appeal any portion of this plan. I understand that the purpose of this plan is to identify my or my family’s strengths, needs, preferences, and resources to help promote a positive quality of life. I understand that if my needs change, an update to this support plan may be needed. Supports should be identified according to my or my family’s needs regardless of the availability of funds. Supports and services needed to meet my needs will be sought from my personal resources, community resources and government resources. When government resources are necessary, they shall be provided based on the availability of general revenue funds.
Individual’s Signature: |
Date: |
|
Date Copy |
|
|
|
|
Sent: |
|
|
|
|
|
|
|
Date Copy Sent to Area: |
|
||
|
|
|
|
|
Legal Representative’s Signature: |
Date: |
|
Date Copy |
|
|
|
|
Sent: |
|
|
|
|
|
|
Printed Name and Telephone Number: |
Relationship (parent, guardian advocate, |
|||
|
POA) |
|
|
|
|
|
|
|
|
Signature of Support Plan Participants
Relationship |
Name /Address/Program (if applicable) |
Date of |
Date Copy |
|
|
Signature |
Sent: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Support Plan Participants: Enter the relationship, and the name(s)/address/program (if applicable) of the individual(s) who are invited by the person and participated in the development of the support plan, and the date the support plan was signed. Provide the date the support plan was provided/mailed to the participant.
FORM TITLE: SUPPORT PLAN/SUPPORT PLAN UPDATE |
YEAR: 4/5/2007 |
FORM NUMBER: