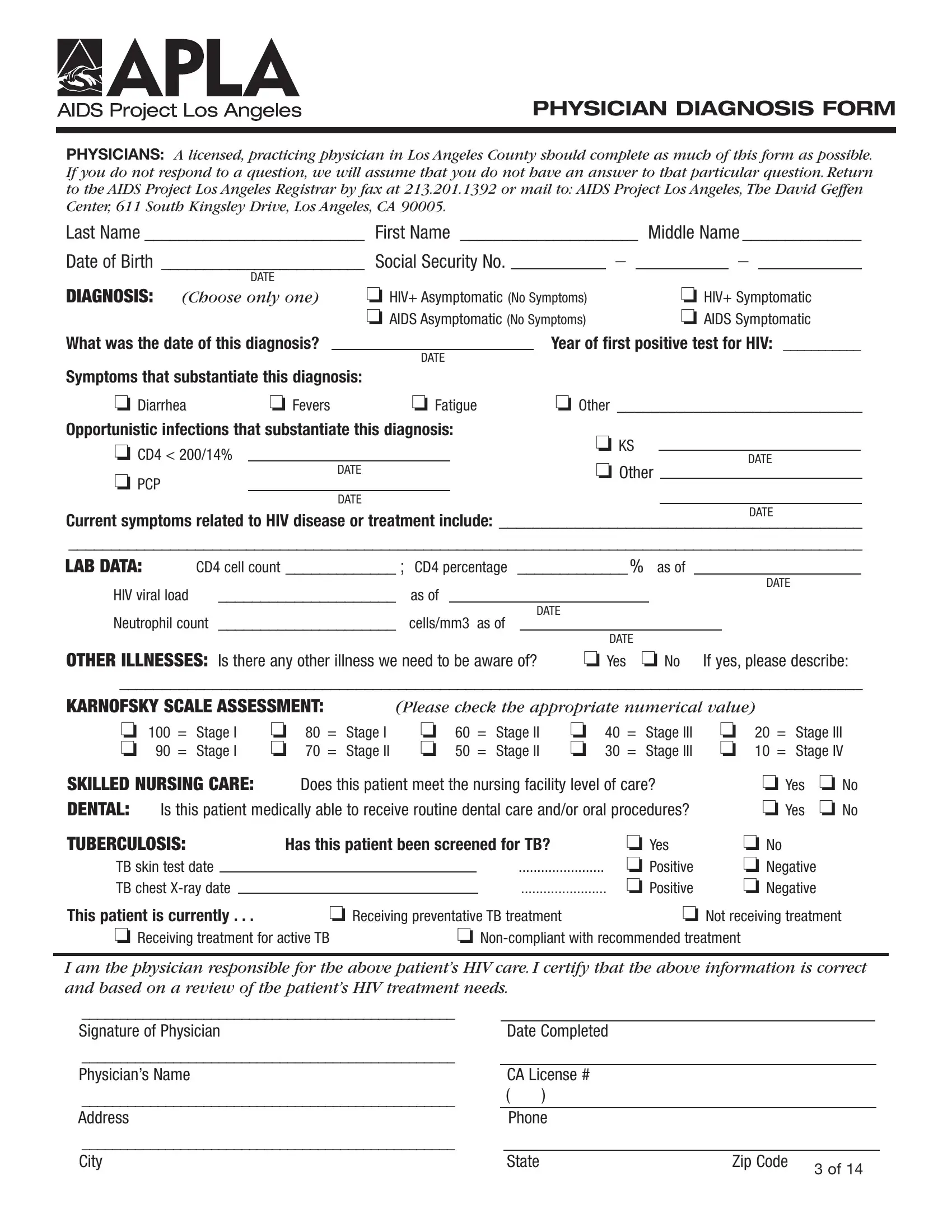
For many individuals living with HIV or AIDS in Los Angeles County, navigating their healthcare journey is complex and often requires detailed documentation to ensure they receive the appropriate care and support. The APLA Diagnosis Form serves as a crucial piece of this intricate puzzle. Designed to be completed by a licensed, practicing physician, this form captures a comprehensive snapshot of a patient's health status, spanning from initial diagnosis, symptomatology, to relevant lab data and necessary care assessments. Patients' basic identification details are meticulously recorded alongside critical diagnostic information, such as the date of HIV or AIDS diagnosis, symptom presence, opportunistic infections, and key lab data like CD4 cell counts and HIV viral load. Additionally, the form delves into other illness considerations that could impact patient care, the Karnofsky Scale Assessment for determining patient capability, and queries on skilled nursing care requirements, dental health, and tuberculosis screening. Ensuring each question is approached with the utmost care, physicians contribute significantly to the care continuum of individuals grappling with HIV/AIDS, providing a well-rounded view of their medical needs to Aids Project Los Angeles. This organization leverages such detailed forms to channel the right support and resources, ultimately fostering better health outcomes for affected persons in the community.
| Question | Answer |
|---|---|
| Form Name | Apla Diagnosis Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | apla kingsley medical diagnosis form, apla health forms, apla physician diagnosis form, apla karnosky form |
PHYSICIAN DIAGNOSIS FORM
PHYSICIANS: A licensed, practicing physician in Los Angeles County should complete as much of this form as possible. If you do not respond to a question, we will assume that you do not have an answer to that particular question. Return to the AIDS Project Los Angeles Registrar by fax at 213.201.1392 or mail to: AIDS Project Los Angeles, The David Geffen Center, 611 South Kingsley Drive, Los Angeles, CA 90005.
Last Name _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ |
First Name _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ |
Middle Name _ _ _ _ _ _ _ _ _ _ _ _ _ _ |
||||||||
|
|
|
|
|
|
|
|
|
|
|
Date of Birth |
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ |
Social Security No. |
_ |
|
|
_ |
|
|||
|
|
|
|
|
||||||
|
DATE |
|
|
|
|
|
|
|
|
|
DIAGNOSIS: |
❏ HIV+ Asymptomatic (No Symptoms) |
|
|
❏ HIV+ Symptomatic |
||||||
|
|
|||||||||
(Choose only one) |
|
|
||||||||
|
|
|
❏ AIDS Asymptomatic (No Symptoms) |
|
|
❏ AIDS Symptomatic |
||||
What was the date of this diagnosis? |
|
|
|
Year of first positive test for HIV: ___________ |
||||||
|
|
|
DATE |
|
|
|
|
|
||
Symptoms that substantiate this diagnosis:
❏ Diarrhea |
❏ Fevers |
❏ Fatigue |
Opportunistic infections that substantiate this diagnosis:
❏CD4 < 200/14%
DATE
❏PCP
DATE
❏Other _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
❏KS
DATE
❏Other
DATE
Current symptoms related to HIV disease or treatment include: ___________________________________________
______________________________________________________________________________________________
LAB DATA: |
CD4 cell count _ _ _ _ _ _ _ _ _ _ _ _ _ ; |
CD4 percentage _ _ _ _ _ _ _ _ _ _ _ _ _ % as of |
|
|
|
|
|
||||||||||
|
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ |
|
|
|
|
|
|
|
|
|
|
DATE |
|
|
|||
HIV viral load |
as of |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Neutrophil count _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ |
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
||||
cells/mm3 as of |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
OTHER ILLNESSES: Is there any other illness we need to be aware of? |
❏ Yes |
❏ No |
If yes, please describe: |
||||||||||||||
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ |
|||||||||||||||||
KARNOFSKY SCALE ASSESSMENT: |
(Please check the appropriate numerical value) |
|
|
||||||||||||||
❏ 100 = |
Stage I |
❏ |
80 = |
Stage I |
❏ |
60 = |
Stage II |
❏ |
40 = |
Stage III |
❏ |
20 = |
Stage III |
||||
❏ 90 = |
Stage I |
❏ |
70 = |
Stage II |
❏ |
50 = |
Stage II |
❏ |
30 = |
Stage III |
❏ |
10 = |
Stage IV |
||||
SKILLED NURSING CARE: |
Does this patient meet the nursing facility level of care? |
❏ Yes |
❏ No |
|||||||
DENTAL: |
Is this patient medically able to receive routine dental care and/or oral procedures? |
❏ Yes |
❏ No |
|||||||
TUBERCULOSIS: |
Has this patient been screened for TB? |
❏ Yes |
❏ No |
|
||||||
TB skin test date |
|
|
|
|
|
....................... |
❏ Positive |
❏ Negative |
|
|
TB chest |
|
|
|
|
....................... |
❏ Positive |
❏ Negative |
|
||
This patient is currently . . . |
❏ Receiving preventative TB treatment |
❏ Not receiving treatment |
||||||||
❏ Receiving treatment for active TB |
❏ |
|
|
|||||||
I am the physician responsible for the above patient’s HIV care. I certify that the above information is correct and based on a review of the patient’s HIV treatment needs.
_________________________________________________ |
|
|
|
|
|
Signature of Physician |
|
Date Completed |
|
|
|
_________________________________________________ |
|
|
|
|
|
Physician’s Name |
|
CA License # |
|
|
|
_________________________________________________ |
( |
) |
|
|
|
Address |
|
Phone |
|
|
|
_________________________________________________ |
|
|
|
|
|
City |
|
State |
Zip Code |
3 OF 14 |
|
|
|
|
|
|
|