Our leading computer programmers have worked together to implement the PDF editor that you may begin using. This application makes it easy to complete ash authorization form forms immediately and effortlessly. This is certainly everything you should undertake.
Step 1: Select the button "Get Form Here" on the following website and click it.
Step 2: Once you've entered the editing page ash authorization form, you should be able to find each of the options readily available for your document in the top menu.
The next areas will create the PDF file that you'll be creating:
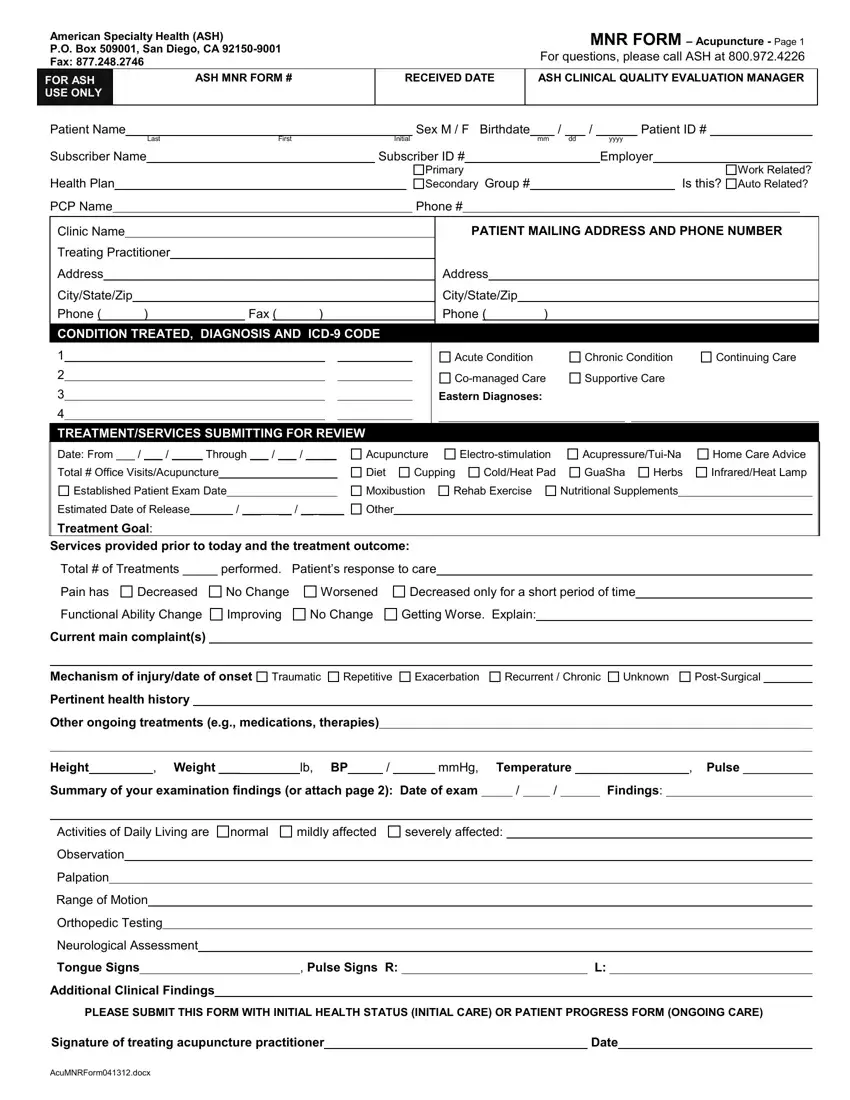
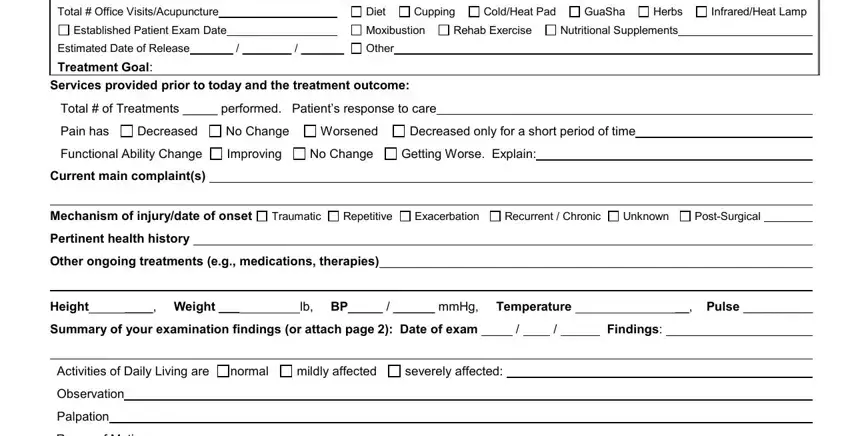
The system will demand you to fill out the Total, Office, Visits, Acupuncture Established, Patient, Exam, Date Diet, Cupping, Cold, Heat, Pad Gua, Sha Herbs, Infrared, Heat, Lamp Mox, i, bust, ion Rehab, Exercise Nutritional, Supplements Estimated, Date, of, Release Other, Treatment, Goal and Pain, has section.
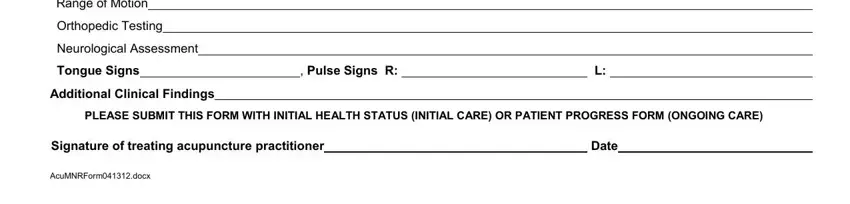
Describe the main details about the Range, of, Motion Orthopedic, Testing Neurological, Assessment Tongue, Signs Pulse, Signs, R Additional, Clinical, Findings Date, and A, cuM, NR, Form, do, cx section.
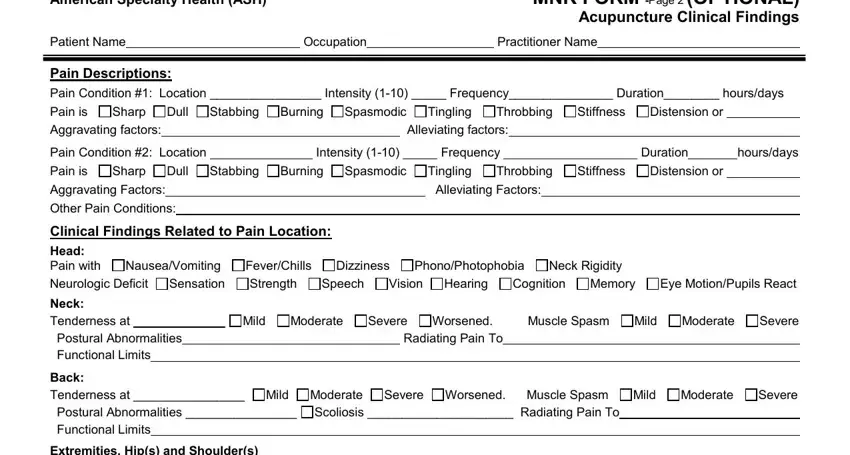
The Patient, Name Pain, Descriptions Occupation, Practitioner, Name Aggravating, factors Alleviating, factors Pain, Condition, Location Intensity, Frequency, Duration, hours, days Aggravating, Factors Other, Pain, Conditions Alleviating, Factors and Radiating, Pain, To area is the place where each party can put their rights and responsibilities.
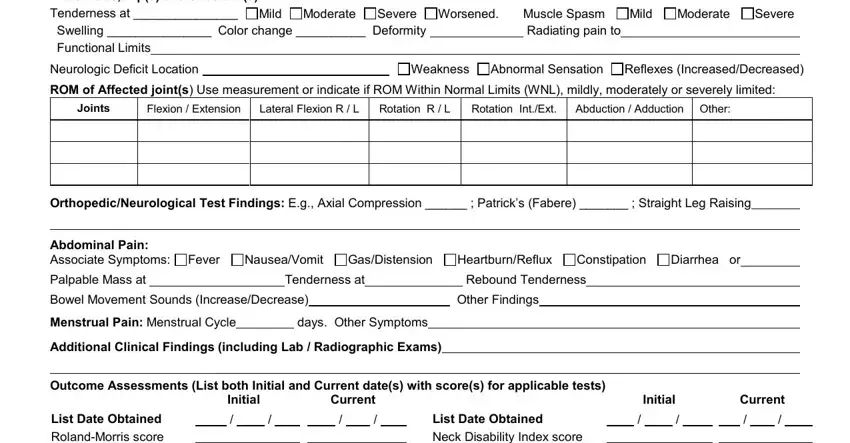
Finish by looking at the next sections and filling them out as needed: Extremities, Hips, and, Shoulders Joints, Flex, ion, Extension Lateral, Flex, ion, RL Rotation, RL Rotation, In, tExt Abduction, Adduct, ion, Other Palpable, Mass, at Tenderness, at Rebound, Tenderness Bowel, Movement, Sounds, Increase, Decrease Other, Findings Menstrual, Pain, Menstrual, Cycle days, Other, Symptoms and Initial.
Step 3: Hit the button "Done". Your PDF document may be exported. You can easily upload it to your device or send it by email.
Step 4: Make sure to remain away from forthcoming problems by creating minimally a pair of copies of the form.
