

You are able to work with asi treatment plan sample instantly by using our online tool for PDF editing. To make our editor better and less complicated to use, we constantly design new features, considering suggestions coming from our users. For anyone who is seeking to start, here's what it takes:
Step 1: Open the form inside our tool by clicking the "Get Form Button" above on this page.
Step 2: With our state-of-the-art PDF editing tool, you are able to accomplish more than just fill out blank fields. Edit away and make your documents look professional with customized textual content put in, or adjust the original content to excellence - all comes with an ability to insert any type of photos and sign the PDF off.
With regards to the fields of this precise PDF, this is what you want to do:
1. When submitting the asi treatment plan sample, make certain to include all necessary blank fields within the associated part. This will help to facilitate the work, which allows your information to be handled swiftly and accurately.
2. The subsequent step would be to submit these particular blanks: Interventions What will the, Participation in Treatment, Participation by Others in the, Note All participants may not have, and Counselor SignatureDate.
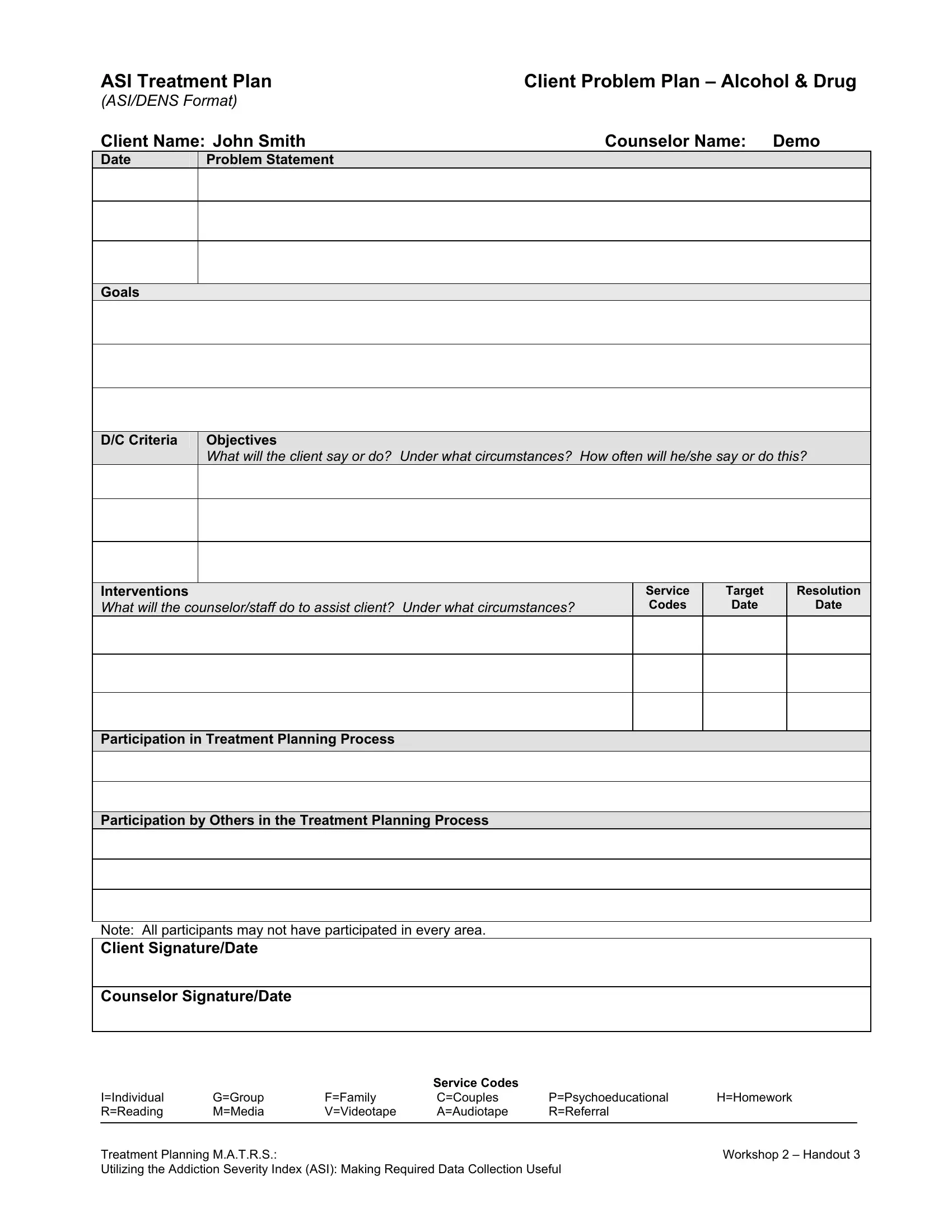
3. Your next step is generally easy - complete all the fields in ASI Treatment Plan ASIDENS Format, Problem Statement, Counselor Name Demo, Goals, DC Criteria, Objectives What will the client, Service Codes, Target Date, Resolution, Date, and Interventions What will the to complete this segment.
4. The subsequent subsection needs your information in the subsequent places: Participation in Treatment, Participation by Others in the, Note All participants may not have, and Counselor SignatureDate. Be sure you provide all required information to move onward.
Concerning Note All participants may not have and Counselor SignatureDate, be certain you do everything right here. These two are viewed as the most important fields in this document.
5. This form has to be concluded within this part. Here you can see a comprehensive set of fields that need specific information for your form submission to be faultless: ASI Treatment Plan ASIDENS Format, Problem Statement, Counselor Name Demo, Goals, DC Criteria, Objectives What will the client, Service Codes, Target Date, Resolution, Date, and Interventions What will the.
Step 3: Make sure that your details are correct and then click on "Done" to conclude the process. Get hold of the asi treatment plan sample after you join for a 7-day free trial. Instantly access the pdf in your personal account, together with any modifications and adjustments all preserved! Whenever you work with FormsPal, you can certainly fill out forms without stressing about data incidents or records getting shared. Our secure system ensures that your private information is stored safe.