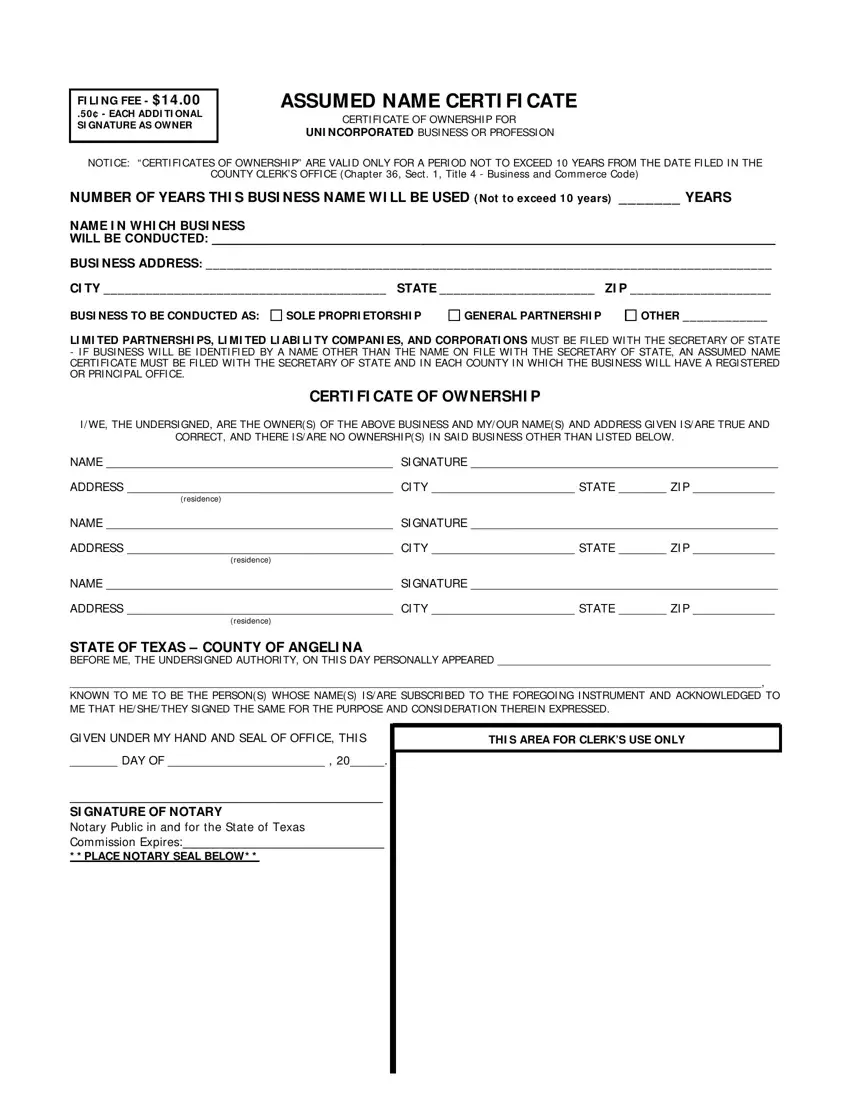
FI LI NG FEE - $ 1 4 .0 0
.50 ¢ - EACH ADDI TI ONAL SI GNATURE AS OWNER
ASSUMED NAME CERTI FI CATE
CERTI FI CATE OF OWNERSHI P FOR
UNI NCORPORATED BUSI NESS OR PROFESSI ON
NOTI CE: “ CERTI FI CATES OF OWNERSHI P” ARE VALI D ONLY FOR A PERI OD NOT TO EXCEED 10 YEARS FROM THE DATE FI LED I N THE
COUNTY CLERK’S OFFI CE (Chapter 36, Sect . 1, Title 4 - Business and Commerce Code)
NUMBER OF YEARS THI S BUSI NESS NAME WI LL BE USED ( Not to exceed 10 years) _______ YEARS
NAME I N WHI CH BUSI NESS
WILL BE CONDUCTED: _________________________________________________________________________________
BUSI NESS ADDRESS: ________________________________________________________________________________
CI TY ________________________________________ STATE ______________________ ZI P ____________________
BUSI NESS TO BE CONDUCTED AS:
LI MI TED PARTNERSHI PS, LI MI TED LI ABI LI TY COMPANI ES, AND CORPORATI ONS MUST BE FI LED WI TH THE SECRETARY OF STATE
-I F BUSI NESS WI LL BE I DENTI FI ED BY A NAME OTHER THAN THE NAME ON FI LE WI TH THE SECRETARY OF STATE, AN ASSUMED NAME CERTI FI CATE MUST BE FI LED WI TH THE SECRETARY OF STATE AND I N EACH COUNTY I N WHI CH THE BUSI NESS WI LL HAVE A REGI STERED OR PRI NCI PAL OFFI CE.
CERTI FI CATE OF OWNERSHI P
I / WE, THE UNDERSI GNED, ARE THE OWNER(S) OF THE ABOVE BUSI NESS AND MY/ OUR NAME(S) AND ADDRESS GI VEN I S/ ARE TRUE AND
CORRECT, AND THERE I S/ ARE NO OWNERSHI P(S) I N SAI D BUSI NESS OTHER THAN LI STED BELOW.
NAME __________________________________________ SI GNATURE _____________________________________________
ADDRESS _______________________________________ CI TY _____________________ STATE _______ ZI P ____________
(residence)
NAME __________________________________________ SI GNATURE _____________________________________________
ADDRESS _______________________________________ CI TY _____________________ STATE _______ ZI P ____________
(residence)
NAME __________________________________________ SI GNATURE _____________________________________________
ADDRESS _______________________________________ CI TY _____________________ STATE _______ ZI P ____________
(residence)
STATE OF TEXAS – COUNTY OF ANGELI NA
BEFORE ME, THE UNDERSI GNED AUTHORI TY, ON THI S DAY PERSONALLY APPEARED _____________________________________________
__________________________________________________________________________________________________________________,
KNOWN TO ME TO BE THE PERSON(S) WHOSE NAME(S) I S/ ARE SUBSCRI BED TO THE FOREGOI NG I NSTRUMENT AND ACKNOWLEDGED TO ME THAT HE/ SHE/ THEY SI GNED THE SAME FOR THE PURPOSE AND CONSI DERATI ON THEREI N EXPRESSED.
GI VEN UNDER MY HAND AND SEAL OF OFFI CE, THI S
_______ DAY OF _______________________ , 20_____.
_____________________________________________
SI GNATURE OF NOTARY
Notary Public in and for the State of Texas
Commission Expires:_____________________________
* * PLACE NOTARY SEAL BELOW* *
THI S AREA FOR CLERK’S USE ONLY