


Should you would like to fill out cg claim form pdf, there's no need to download and install any sort of applications - simply make use of our PDF editor. Our editor is constantly evolving to deliver the best user experience possible, and that is thanks to our resolve for constant improvement and listening closely to user feedback. For anyone who is looking to begin, this is what it's going to take:
Step 1: Click on the orange "Get Form" button above. It'll open up our pdf tool so you can start filling out your form.
Step 2: The tool gives you the ability to customize PDF files in various ways. Change it by including any text, correct what is originally in the document, and include a signature - all when you need it!
This form will need some specific details; in order to guarantee accuracy and reliability, please be sure to take heed of the suggestions further down:
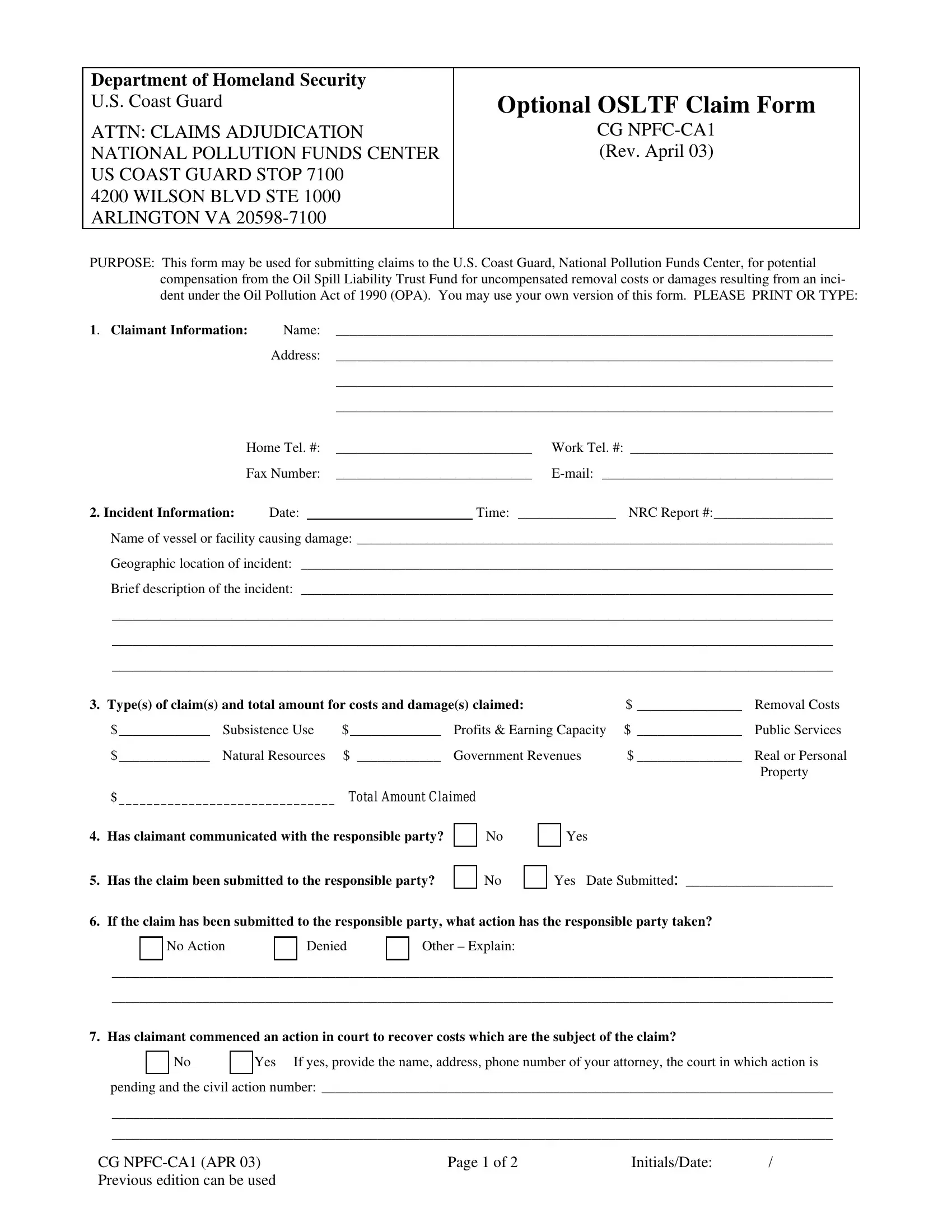
1. Complete your cg claim form pdf with a number of major blanks. Consider all the required information and ensure absolutely nothing is left out!
2. After performing this step, go on to the subsequent stage and complete all required details in all these blanks - Types of claims and total amount, Subsistence Use Profits , Natural Resources Government, Property, Total Amount Claimed, Has claimant communicated with, Has the claim been submitted to, If the claim has been submitted, No Action, Denied, Other Explain, Has claimant commenced an action, Yes If yes provide the name, pending and the civil action, and CG NPFCCA APR Previous edition.
3. This subsequent part is rather easy, Has claimant submitted or planned, the name address and phone number, Description of the nature and, Description of how the incident, Description of actions taken by, Witnesses, Name Tel No , Address , Name Tel No , and Address - all these empty fields is required to be filled in here.
Many people often make mistakes while filling out Address in this section. Don't forget to read twice what you enter right here.
4. This particular part comes with the following form blanks to complete: Address , List Documents or Attachments, I the undersigned agree that upon, I the undersigned certify that to, Claimants Signature, Date, Printed Name of Signer, TitleLegal Capacity, Legal Representative, and Date.
Step 3: Soon after looking through the fields and details, press "Done" and you're good to go! Obtain the cg claim form pdf when you register here for a 7-day free trial. Conveniently access the pdf within your personal account, with any edits and changes all preserved! FormsPal guarantees your data privacy with a secure system that never records or shares any type of personal data involved. Rest assured knowing your files are kept protected every time you use our service!