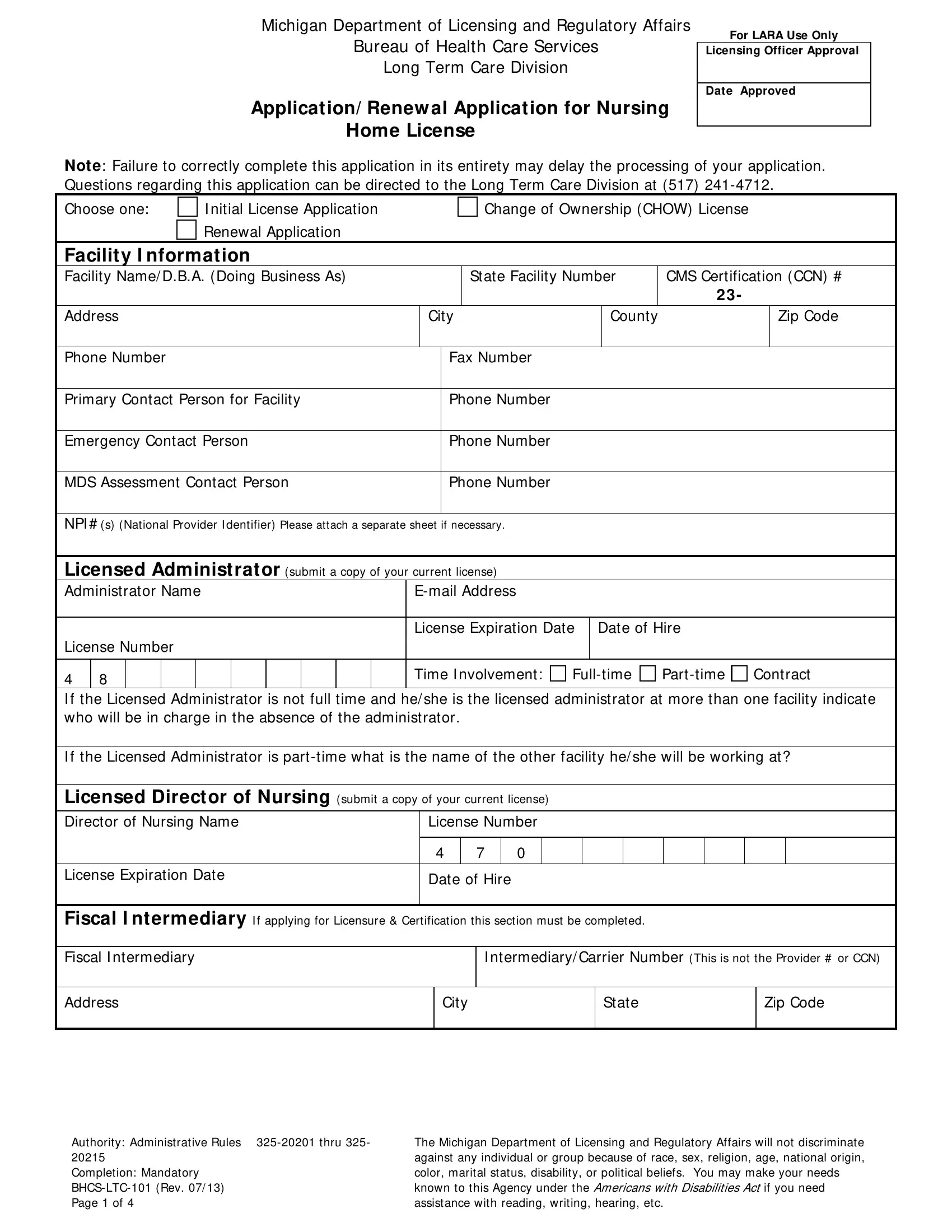
The BHCS LTC 101 form, issued by the Michigan Department of Licensing and Regulatory Affairs Bureau of Health Care Services Long Term Care Division, serves as an essential document for nursing homes within Michigan seeking to apply for, or renew, their license. This comprehensive application encompasses several key areas including the initial application for a new license, changes in ownership, and the renewal of an existing license. It requires detailed information about the nursing home facility, including but not limited to, facility name, address, contact details, bed information, and specific sections dedicated to the licensed administrator and director of nursing. Additionally, the form delves into fiscal intermediary details, ownership data, and information regarding officers, directors, and trustees, emphasizing on the necessity for transparency and thoroughness to ensure proper processing. Special sections also inquire about the facility's affiliations, criminal history of its managing employees, and interests in other healthcare facilities, aiming to ensure compliance with federal and state regulations. Not to be overlooked, the form stipulates the importance of acknowledging the assistance available under the Americans with Disabilities Act for those needing help with the application process. Completing this form accurately and completely is vital, as any inaccuracies or omissions may not only delay the process but could also lead to the denial of licensure, underlining the form’s crucial role in maintaining the standards and regulatory compliance of nursing homes in Michigan.
| Question | Answer |
|---|---|
| Form Name | Bhcs Ltc 101 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | CCN, MDS, bchs ltc 101, LARA |
Michigan Department of Licensing and Regulatory Affairs
Bureau of Health Care Services
Long Term Care Division
Application/ Renew al Application for Nursing Home License
For LARA Use Only
Licensing Officer Approval
Date Approved
Not e: Failure to correctly complete this application in its entirety may delay the processing of your application. Questions regarding this application can be directed to the Long Term Care Division at (517)
Choose one: |
I nitial License Application |
|
|
Change of Ownership (CHOW) License |
|||
|
Renewal Application |
|
|
|
|
|
|
Facility I nformation |
|
|
|
|
|
|
|
Facility Name/ D.B.A. (Doing Business As) |
|
|
State Facility Number |
CMS Certification (CCN) # |
|||
|
|
|
|
|
|
23 - |
|
Address |
|
City |
County |
|
Zip Code |
||
|
|
|
|
|
|
|
|
Phone Number |
|
|
Fax Number |
|
|
|
|
|
|
|
|
|
|
||
Primary Contact Person for Facility |
|
Phone Number |
|
|
|
||
|
|
|
|
|
|
||
Emergency Contact Person |
|
Phone Number |
|
|
|
||
|
|
|
|
|
|
||
MDS Assessment Contact Person |
|
Phone Number |
|
|
|
||
|
|
|
|
|
|
|
|
NPI # (s) (National Provider I dentifier) Please attach a separate sheet if necessary.
Licensed Administrator (submit a copy of your current license)
Administrator Name |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
License Expiration Date |
Date of Hire |
|
||
License Number |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
8 |
|
|
|
|
|
|
|
|
Time I nvolvement: |
Part |
Contract |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
I f the Licensed Administrator is not full time and he/ she is the licensed administrator at more than one facility indicate who will be in charge in the absence of the administrator.
I f the Licensed Administrator is part
Licensed Director of Nursing (submit a copy of your current license)
Director of Nursing Name |
License Number |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
7 |
|
0 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
License Expiration Date |
Date of Hire |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||||
Fiscal I ntermediary I f applying for Licensure & Certification this section must be completed. |
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|||||||||
Fiscal I ntermediary |
|
|
|
I ntermediary/ Carrier Number (This is not the Provider # or CCN) |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Address |
|
City |
|
|
|
|
|
State |
|
|
|
Zip Code |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Authority: Administrative Rules |
The Michigan Department of Licensing and Regulatory Affairs will not discriminate |
20215 |
against any individual or group because of race, sex, religion, age, national origin, |
Completion: Mandatory |
color, marital status, disability, or political beliefs. You may make your needs |
known to this Agency under the Americans with Disabilities Act if you need |
|
Page 1 of 4 |
assistance with reading, writing, hearing, etc. |
Michigan Department of Licensing and Regulatory Affairs
Bureau of Health Care Services
Long Term Care Division
Bed I nformation ( current or requested beds)
|
|
|
|
|
|
|
|
|
|
|
|
Current Beds |
|
Requested Beds |
|
Does the facility have any of the following |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
beds that are not part of the “ Special |
|||||
Medicare (SNF) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pool Beds” issued by Certificate of Need? |
||||||||||||||||
Medicaid (NF) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Religious Beds |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ventilator Dependent |
||||
Medicare/ Medicaid (SNF/ NF) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dialysis |
|
|||||||||||||
Total Certified Beds: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Alzheimer’s Beds |
|
|||||||||||||||
Licensed Only Beds* : |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hospice |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Total Facility Beds: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
* Fees are for the billing cycle covering the period of 8/ 1 through 7/ 31. |
|
|
|
|
|
|
|
||||||||||||||||||||||||||
Change of Ownership fees is equal to 1 year license fee regardless of the |
|
|
|
|
|
|
|
||||||||||||||||||||||||||
billing cycle. DO NOT SEND FEES W I THOUT RECEI VI NG AN I NVOI CE. |
|
|
|
|
|
|
|
||||||||||||||||||||||||||
Does the facility have a locked Unit? |
I f yes, what special population is serving that unit? |
|
|||||||||||||||||||||||||||||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Ow nership (legal entity which directly owns the facility) |
|
|
|
|
|
|
|||||||||||||||||||||||||||
Company/ Owner Legal Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary Owner |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Phone Number |
Fax Number |
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
State |
|
Zip Code |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Tax I D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I s the Ownership for: |
|
Does the Owner |
|
||||||||||
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Profit |
|
Own the building |
or |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Non Profit |
|
I s this a management company |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Type of Entity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Profit I ndividual |
|
|
Non Profit Religious |
|
|
|
State |
|
|
|
City/ County |
|
|||||||||||||||||||||
Profit Partnership |
|
|
Non Profit Corporation |
|
|
County |
|
|
|
Hospital District |
|||||||||||||||||||||||
Profit Corporation |
|
|
Non Profit Other |
|
|
|
City |
|
|
|
Federal |
|
|||||||||||||||||||||
I s the applicant part of a nursing home chain? |
|
I f yes, does this chain own |
|
|
|
||||||||||||||||||||||||||||
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
More than 30 |
|
|
|
Less than 30 |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Parent Organization Name |
|
|
|
|
|
|
|
|
|
|
Contact Person |
|
|
|
|
Phone Number |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
|
Zip Code |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Tax I D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Contact Name |
|
|
|
|
|||||||||
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Authority: Administrative Rules |
The Michigan Department of Licensing and Regulatory Affairs will not discriminate |
20215 |
against any individual or group because of race, sex, religion, age, national origin, |
Completion: Mandatory |
color, marital status, disability, or political beliefs. You may make your needs |
known to this Agency under the Americans with Disabilities Act if you need |
|
Page 2 of 4 |
assistance with reading, writing, hearing, etc. |
Michigan Department of Licensing and Regulatory Affairs
Bureau of Health Care Services
Long Term Care Division
Officers/ Directors/ Trustees: (attach additional pages if necessary)
Name |
Phone Number |
|
|
Address
Tenure From (date) |
I s Primary |
|
|||||||||
|
|
|
|
|
|
|
|
Yes |
|
||
|
|
|
|
|
|
|
|
No |
|
||
Tax I D |
|
|
|
|
|
|
|||||
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|||||
Address |
|
|
|
|
|
|
|||||
Tenure From (date) |
|
I s Primary |
|
||||||||
|
|
||||||||||
|
|
|
|
|
|
|
|
Yes |
|
||
|
|
|
|
|
|
|
|
No |
|
||
Tax I D |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
||||||
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Name |
|
|
|
|
|
|
|||||
Address |
|
|
|
|
|
|
|||||
|
|
|
|
||||||||
Tenure From (date) |
|
I s Primary |
|
||||||||
|
|
|
|
|
|
|
|
Yes |
|
||
|
|
|
|
|
|
|
|
No |
|
||
|
|
|
|
|
|
|
|||||
Tax I D |
|
|
|
|
|
|
|||||
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Name |
|
|
|
|
|
|
|||||
Address |
|
|
|
|
|
|
|||||
|
|
|
|
||||||||
Tenure From (date) |
|
I s Primary |
|
||||||||
|
|
|
|
|
|
|
|
Yes |
|
||
|
|
|
|
|
|
|
|
No |
|
||
|
|
|
|
|
|
|
|||||
Tax I D |
|
|
|
|
|
|
|||||
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
|
Zip Code |
|||||||
ion |
|
|
Director |
|
|
Manager |
|
|
President |
||||||
|
|
|
|
|
|
||||||||||
|
|
Secretary |
|
|
Treasurer |
|
|
Vice President |
|||||||
Posit |
|
|
|
|
|
|
|||||||||
|
|
Senior Officer |
|
|
Junior Officer |
|
|
Principal Officer |
|||||||
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
Percentage Owned |
|
|
|
|
|||
|
|
|
|
|
|
|
|
Phone Number |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
City |
|
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
ion |
|
|
Director |
|
|
Manager |
|
|
President |
||||||
|
|
Secretary |
|
|
Treasurer |
|
|
Vice President |
|||||||
Posit |
|
|
|
|
|
|
|||||||||
|
|
Senior Officer |
|
|
Junior Officer |
|
|
Principal Officer |
|||||||
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
Percentage Owned |
|
|
||||
|
|
|
|
|
|
|
|
|
Phone Number |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
City |
|
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
|||||||||
ion |
|
|
Director |
|
|
|
Manager |
|
|
|
President |
||||
|
|
|
|
|
|
|
|
||||||||
|
|
Secretary |
|
|
|
Treasurer |
|
|
|
Vice President |
|||||
Posit |
|
|
|
|
|
|
|
|
|||||||
|
|
Senior Officer |
|
|
|
Junior Officer |
|
Principal Officer |
|||||||
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
Percentage Owned |
|
|
||||
|
|
|
|
|
|
|
|
|
Phone Number |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
City |
|
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
|||||||||
ion |
|
|
Director |
|
|
|
Manager |
|
|
|
President |
||||
|
|
|
|
|
|
|
|
||||||||
|
|
Secretary |
|
|
|
Treasurer |
|
|
|
Vice President |
|||||
Posit |
|
|
|
|
|
|
|
|
|||||||
|
|
Senior Officer |
|
|
|
Junior Officer |
|
Principal Officer |
|||||||
|
|
|
|
|
|
|
|||||||||
Percentage Owned
Are there any directors, officers, agents, or managing employees of the institution agency or organization who have
been convicted of a criminal offense? |
No |
Yes → I f “yes”, please attach an additional sheet describing the event . |
Does anyone listed own or have an interest in other healthcare facilities (for example: sole proprietor, partner, member of a
partnership, board of directors)? No Yes → I f “yes”, please attach an additional sheet indicating name, address, city, state & zip code and interest of parent corporation.
I s the applicant facility chain affiliated?
No
Yes → I f “ yes” , please attach an additional sheet indicating name, address, city, state & zip code.
Are any persons who have ownership interest required to file a beneficial ownership report pursuant to the Federal
Securities Exchanges Act of 1934 [ 15 U.S.C. 78p, Sec. 16 (a)] ?
Yes – I f yes, attach copies of such report
No
Authority: Administrative Rules |
The Michigan Department of Licensing and Regulatory Affairs will not discriminate |
20215 |
against any individual or group because of race, sex, religion, age, national origin, |
Completion: Mandatory |
color, marital status, disability, or political beliefs. You may make your needs |
known to this Agency under the Americans with Disabilities Act if you need |
|
Page 3 of 4 |
assistance with reading, writing, hearing, etc. |
Michigan Department of Licensing and Regulatory Affairs
Bureau of Health Care Services
Long Term Care Division
Building Ow ner
Legal Owner of Building |
|
Phone Number |
|
|
|
|
|
|
|
Address |
City |
|
State |
Zip Code |
|
|
|
|
|
Lien Holder (if different from building owner) |
|
|
|
|
Lien Holder
Address
Phone Number
City |
State |
Zip Code |
|
|
|
Management Company (who is responsible for nursing home day to day operations, if different than applicant?)
Name of Company |
Phone Number |
|
|
Address
City
State
Zip Code
Contact Person
PLEASE ONLY COMPLETE THE ESTI MATED MONTHLY REVENUES/ EXPENDI TURES AND PROVI DE THE LI ST OF SUPPLI ERS I F YOU ARE REQUESTI NG AN I NI TI AL LI CENSE FOR THE NURSI NG HOME OR I F YOU HAVE A CHANGE OF OW NERSHI P. NEI THER OF THESE TWO AREAS NEED TO BE COMPLETED I F THI S I S A RENEWAL APPLI CATI ON.
Estimated Monthly Revenues/ Expenditures:
Business experience related to nursing home operation, delivery of health care services:
Estimated monthly revenues:
Estimated monthly expenditures:
List of Suppliers
A list disclosing the names & addresses of each supplier who furnishes goods or services to the nursing home must be attached to this application. You must also include their total charges exceeding $5,000.00 in a 12 month period including a month in the nursing homes current fiscal year.
Certification of Applicant
The Assurance and processing of this form is governed by Administrative Rules 325.20201 through 325.20215. Failure to submit an accurate and complete form in a timely manner may result in denial of licensure or certification. An applicant who makes a false statement in this application is subject to criminal penalties under Section 20142(5) of the Public Health Code (P.A. 368 of 1978 as amended) including four years imprisonment and/ or $30,000 fine. Each facility must be brought in full regulatory compliance at the time a CHOW is approved.
The applicant certifies that the information provided on this application is true, complete and accurate to the best of his/ her knowledge.
The applicant certifies that the applicant and/ or owner(s) have not had a professional, occupational or health agency license revoked within the preceding five years.
Applicant’s Signature |
Applicant’s Title |
Date |
For an I nitial License or Change of Ow nership request please submit the completed form to:
Michigan Department of Licensing and Regulatory Affairs/ BHCS/ Long Term Care Division
Ottawa Building, 1st Floor
P. O. Box 30664
Lansing, MI 48909
Authority: Administrative Rules |
The Michigan Department of Licensing and Regulatory Affairs will not discriminate |
20215 |
against any individual or group because of race, sex, religion, age, national origin, |
Completion: Mandatory |
color, marital status, disability, or political beliefs. You may make your needs |
known to this Agency under the Americans with Disabilities Act if you need |
|
Page 4 of 4 |
assistance with reading, writing, hearing, etc. |