Our finest software engineers worked hard to implement the PDF editor we are now happy to present to you. The application makes it possible to shortly create louisiana medicaid application form and can save your time. You just have to follow this specific instruction.
Step 1: The initial step should be to press the orange "Get Form Now" button.
Step 2: The document editing page is currently available. You can add information or update current content.
Complete the particular areas to fill in the document:
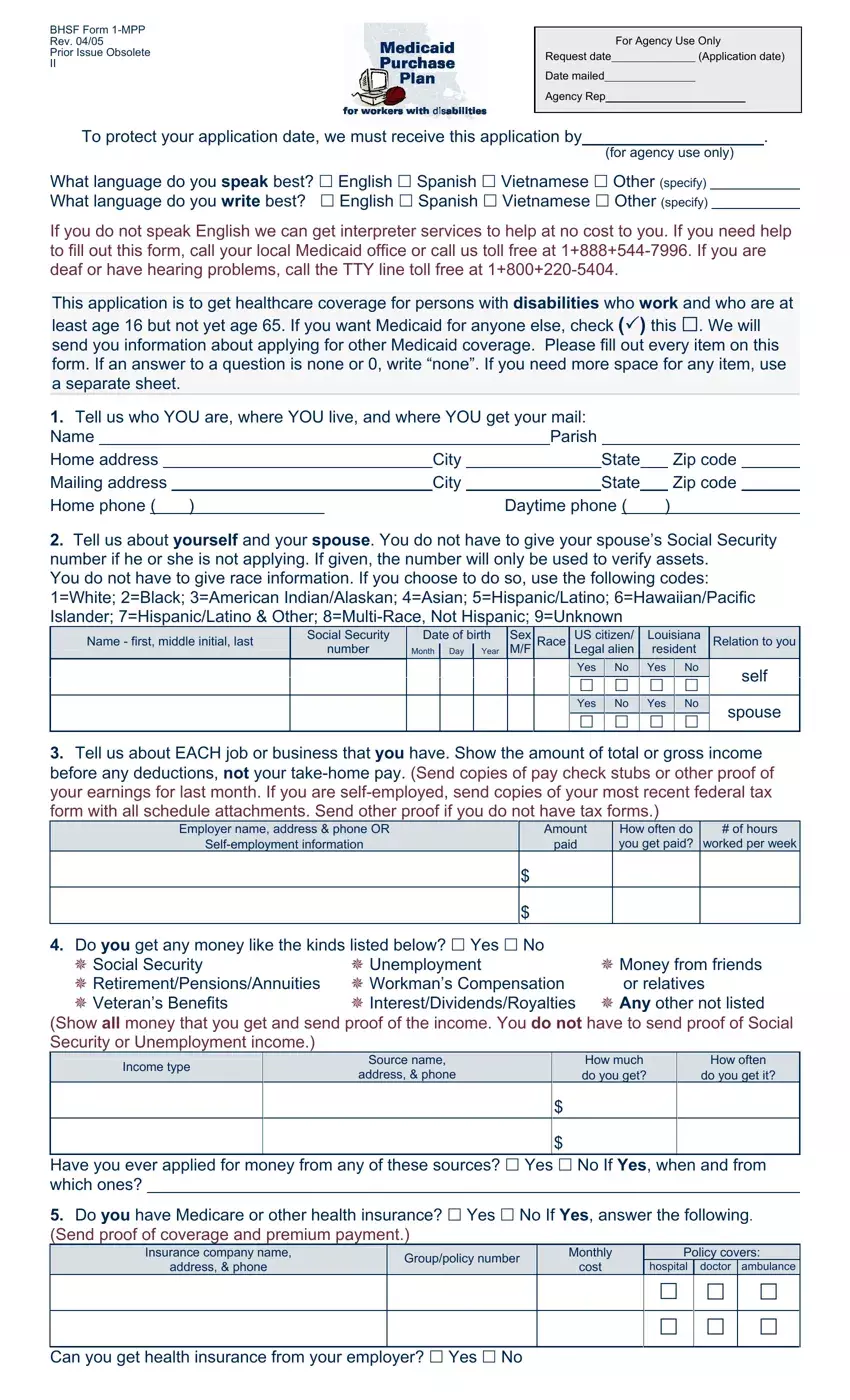
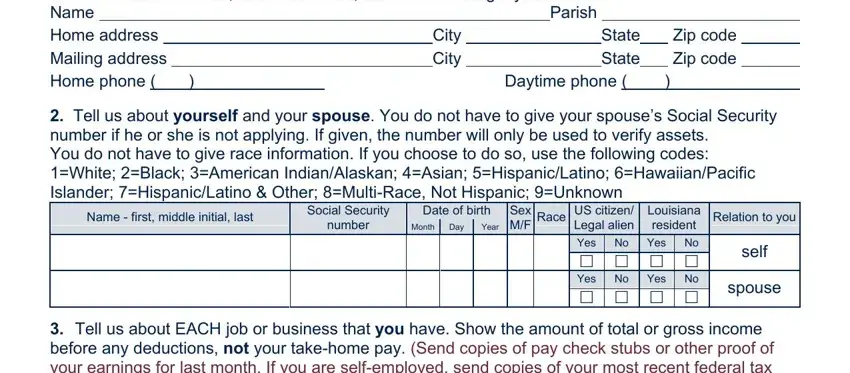
Remember to fill in the Tell us who YOU are where YOU, Daytime phone, Tell us about yourself and your, Name first middle initial last, Social Security number, Date of birth Day, Year, Month, Sex MF, Race, US citizen Legal alien, Louisiana resident, Relation to you, Yes No Yes No cid cid cid cid Yes, and self field with the requested information.
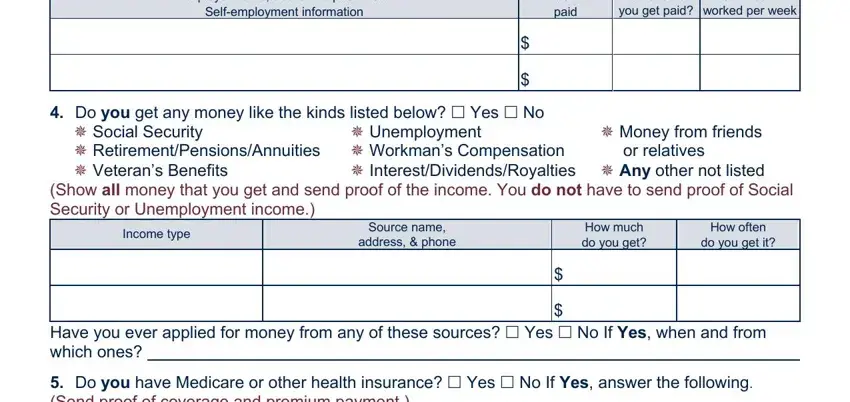
The software will request for additional info to effortlessly fill in the area Employer name address phone OR, Amount paid, How often do you get paid, of hours worked per week, Do you get any money like the, cid InterestDividendsRoyalties cid, cid Money from friends or relatives, cid Unemployment, Income type, Source name address phone, How much do you get, How often do you get it, Have you ever applied for money, and Do you have Medicare or other.
The Insurance company name address, Grouppolicy number, Monthly cost, Policy covers, hospital, doctor ambulance, cid cid cid, cid cid cid, and Can you get health insurance from section will be your place to include the rights and obligations of each side.

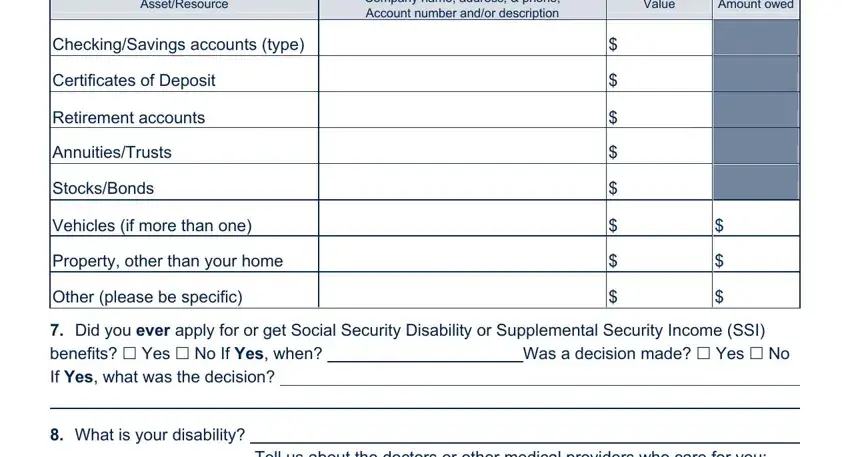
Check the areas AssetResource, Company name address phone, Value, Amount owed, CheckingSavings accounts type, Certificates of Deposit, Retirement accounts, AnnuitiesTrusts, StocksBonds, Vehicles if more than one, Property other than your home, Other please be specific, Did you ever apply for or get, What is your disability, and Tell us about the doctors or other and next fill them out.
Step 3: Select the button "Done". Your PDF file can be transferred. It is possible to save it to your device or email it.
Step 4: Come up with a duplicate of every file. It will certainly save you time and help you avoid troubles as time goes on. By the way, your details will not be revealed or analyzed by us.
