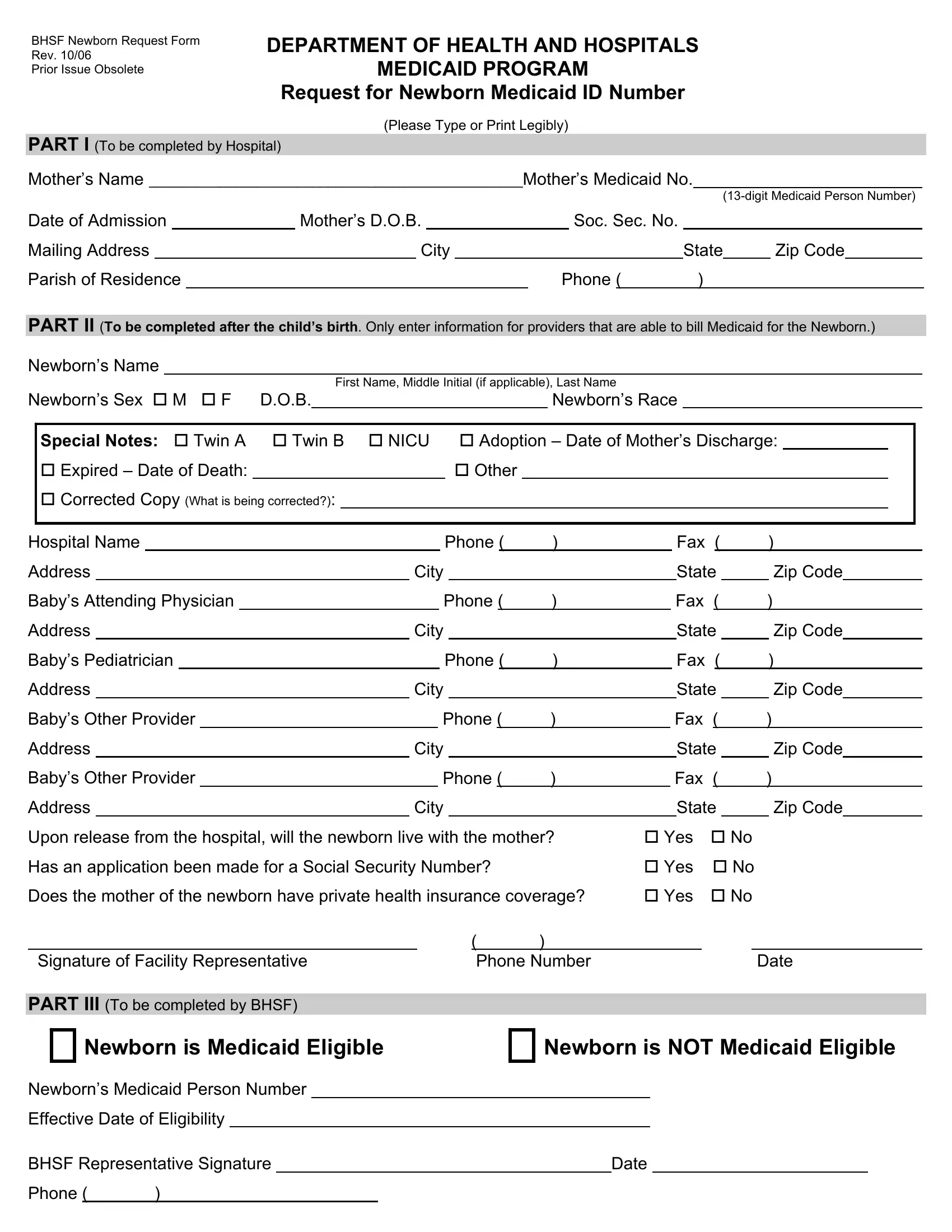
Navigating the complexities of ensuring newborns have timely access to healthcare benefits can pose challenges for new parents and healthcare providers alike. The BHSF Newborn Request Form, an essential document from the Department of Health and Hospitals Medicaid Program, serves as a bridge to secure these crucial benefits. Its main purpose is to request a Medicaid ID number for newborns, ensuring they have access to healthcare without unnecessary delays. The form, revised as of October 2006, with previous issues now obsolete, necessitates detailed input in three distinct parts. Part I, aimed at hospitals, requires the mother's details including her Medicaid number and personal information. Part II kicks in after the baby's birth, asking for the newborn's details and information on healthcare providers capable of billing Medicaid. It also includes provisions for special situations like twins, adoption, or in the unfortunate event, the newborn's passing. Furthermore, questions regarding the baby's living situation post-hospital release and the status of the social security number application are addressed. The process concludes with Part III, filled out by BHSF representatives, which denotes the newborn’s eligibility for Medicaid. Completeness and legibility in filling out this form play a critical role in smoothing the pathway for newborns to receive Medicaid benefits, underscoring the form's significance in the early life stages of healthcare administration.
| Question | Answer |
|---|---|
| Form Name | Bhsf Newborn Request Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names |
BHSF Newborn Request Form
Rev. 10/06
Prior Issue Obsolete
DEPARTMENT OF HEALTH AND HOSPITALS
MEDICAID PROGRAM
Request for Newborn Medicaid ID Number
(Please Type or Print Legibly)
PART I (To be completed by Hospital)
Mother’s Name ________________________________________________Mother’s Medicaid No.
|
|
|
|
|
|
|
|
|
|
|
|
||||
Date of Admission |
|
Mother’s D.O.B. |
|
|
|
Soc. Sec. No. |
|
|
|
|
|
||||
Mailing Address |
|
|
City |
|
|
|
|
State |
|
Zip Code |
|
|
|||
Parish of Residence |
|
|
|
|
|
Phone ( |
) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART II (To be completed after the child’s birth. Only enter information for providers that are able to bill Medicaid for the Newborn.)
Newborn’s Name
|
|
|
|
|
|
|
|
|
First Name, Middle Initial (if applicable), Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Newborn’s Sex M |
|
F |
D.O.B. |
|
|
|
|
|
|
|
|
|
|
Newborn’s Race |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
Special Notes: |
Twin A |
Twin B |
NICU |
|
|
Adoption – Date of Mother’s Discharge: |
|
||||||||||||||||||||||||||
|
Expired – Date of Death: |
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Corrected Copy (What is being corrected?): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hospital Name |
|
|
|
|
|
|
|
|
|
|
|
Phone ( |
) |
|
|
Fax |
( |
) |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Address |
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
|||||||||||
Baby’s Attending Physician |
|
|
|
|
|
|
|
|
Phone ( |
) |
|
Fax |
( |
) |
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Address |
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
||||||||||||
Baby’s Pediatrician |
|
|
|
|
|
|
|
|
|
|
|
Phone ( |
) |
|
|
Fax |
( |
) |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Address |
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
|||||||||||
Baby’s Other Provider |
|
|
|
|
|
|
|
Phone ( |
) |
|
Fax |
( |
) |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Address |
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
||||||||||||
Baby’s Other Provider |
|
|
|
|
|
|
|
Phone ( |
) |
|
Fax |
( |
) |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Address |
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
||||||||||||
Upon release from the hospital, will the newborn live with the mother? |
Yes |
|
|
No |
||||||||||||||||||||||||||||||
Has an application been made for a Social Security Number? |
|
|
Yes |
|
|
No |
||||||||||||||||||||||||||||
Does the mother of the newborn have private health insurance coverage? |
Yes |
|
|
No |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Signature of Facility Representative |
|
|
|
|
|
|
Phone Number |
|
|
|
|
|
|
|
|
Date |
|||||||||||||||||
PART III (To be completed by BHSF)
Newborn is Medicaid Eligible
Newborn is NOT Medicaid Eligible
Newborn’s Medicaid Person Number
Effective Date of Eligibility
BHSF Representative Signature |
|
|
Date |
||
Phone ( |
) |
|
|
|
|
|
|
|
|
|
|