
Using PDF files online is very easy with this PDF tool. You can fill out workers comp c4 form here painlessly. Our tool is constantly evolving to give the best user experience possible, and that's due to our commitment to continual development and listening closely to comments from users. This is what you'll want to do to get going:
Step 1: Press the "Get Form" button above. It'll open up our editor so you could begin completing your form.
Step 2: This editor provides the ability to customize most PDF files in a variety of ways. Change it by including any text, adjust what is originally in the PDF, and put in a signature - all at your convenience!
In an effort to finalize this form, be sure to type in the required information in every single blank:
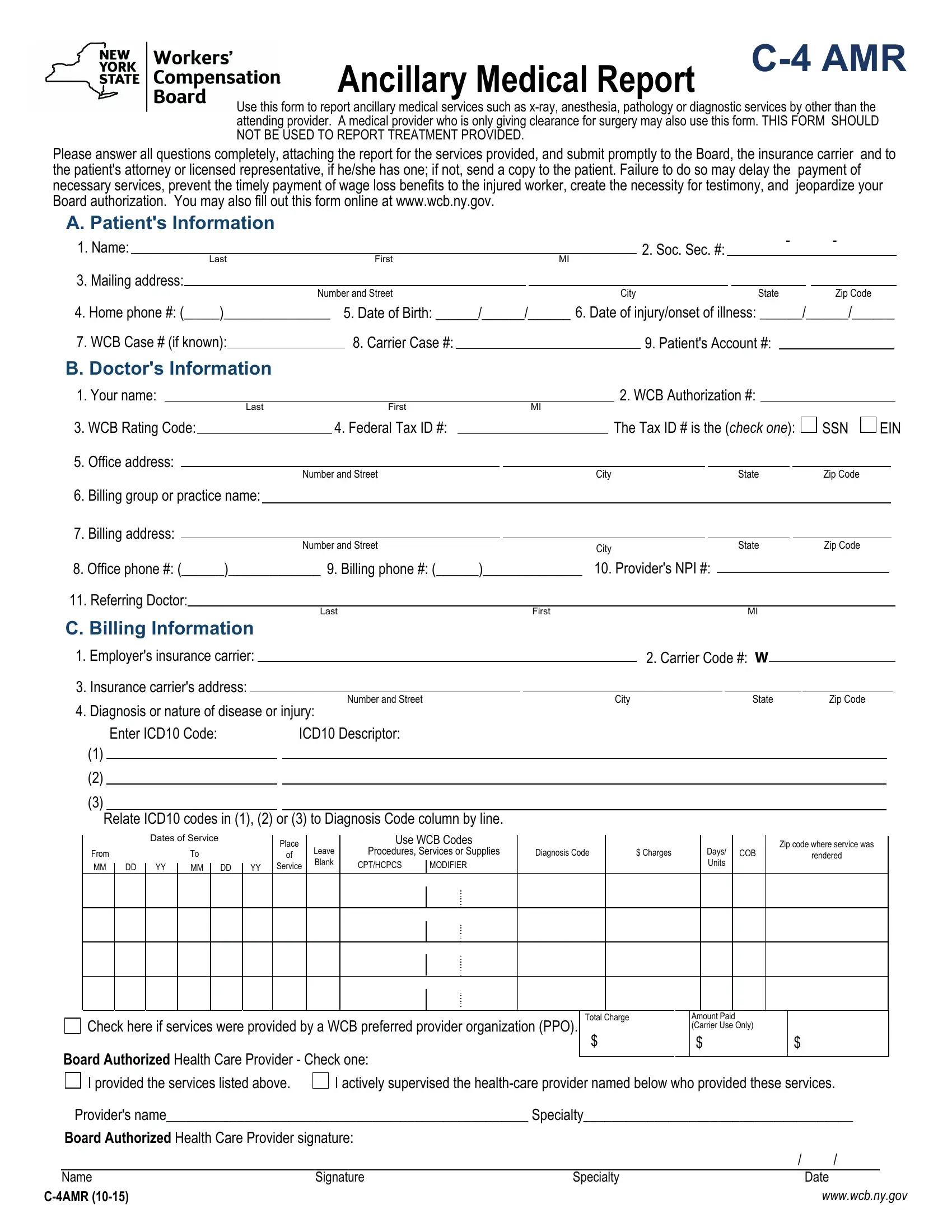
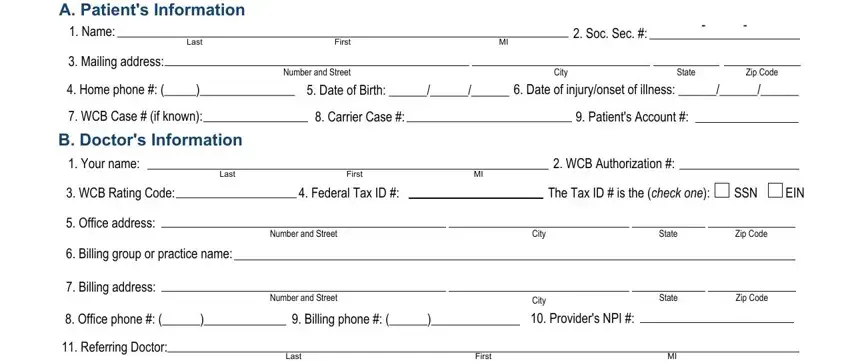
1. Whenever filling in the workers comp c4 form, make sure to include all of the important fields within its associated area. This will help to speed up the process, which allows your details to be processed efficiently and properly.
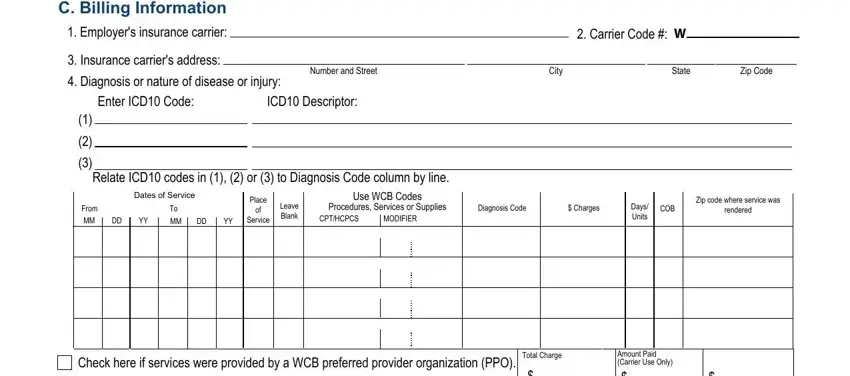
2. Once your current task is complete, take the next step – fill out all of these fields - C Billing Information, Employers insurance carrier, Insurance carriers address, Diagnosis or nature of disease or, Number and Street, City, State, Zip Code, Carrier Code W, Enter ICD Code, ICD Descriptor, Relate ICD codes in or to, Dates of Service, From MM DD YY, and MM DD YY with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. The next step should be rather simple, Board Authorized Health Care, I provided the services listed, I actively supervised the, Providers name Specialty, Board Authorized Health Care, Name, CAMR , Signature, Specialty, Date, and wwwwcbnygov - every one of these fields will have to be filled in here.

4. Now fill in the next form section! In this case you'll get all these C to report continued treatment, C to report permanent impairment, Ophthalmologists use Form C, Please ask your patient for hisher, AUTHORIZATION FOR SPECIAL SERVICES, AUTHORIZATION FOR SPECIAL SERVICES, LIMITATION OF PODIATRY TREATMENT , A CHIROPRACTOR OR PODIATRIST, DEFINED IN THE EDUCATION LAW AND, HIPAA NOTICE In order to, ANY PERSON WHO KNOWINGLY AND WITH, BILLING INFORMATION, IMPORTANT TO THE PATIENT, and YOUR DOCTORS BILLS AND BILLS FOR form blanks to fill in.
Always be really mindful when filling out YOUR DOCTORS BILLS AND BILLS FOR and HIPAA NOTICE In order to, because this is the part in which most people make errors.
Step 3: Reread what you have typed into the blank fields and then hit the "Done" button. After starting afree trial account with us, you'll be able to download workers comp c4 form or email it immediately. The PDF document will also be readily accessible through your personal account menu with all your changes. When using FormsPal, you're able to fill out forms without stressing about information incidents or data entries getting distributed. Our secure system ensures that your private data is stored safely.