

Our top rated developers worked hard to create the PDF editor we are happy to present to you. The application allows you to immediately prepare ca 20 form and will save you valuable time. You just need to follow this specific guide.
Step 1: Choose the button "Get Form Here".
Step 2: So you should be on the form edit page. You can add, transform, highlight, check, cross, insert or erase areas or words.
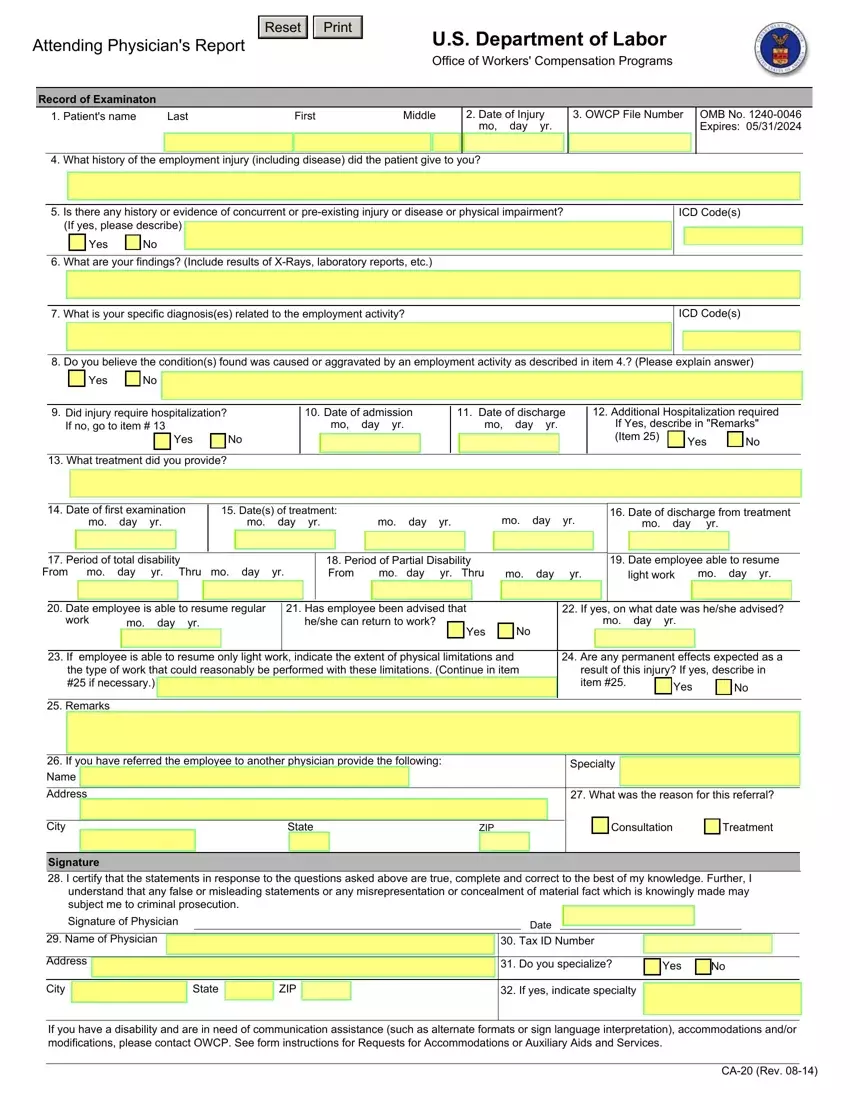
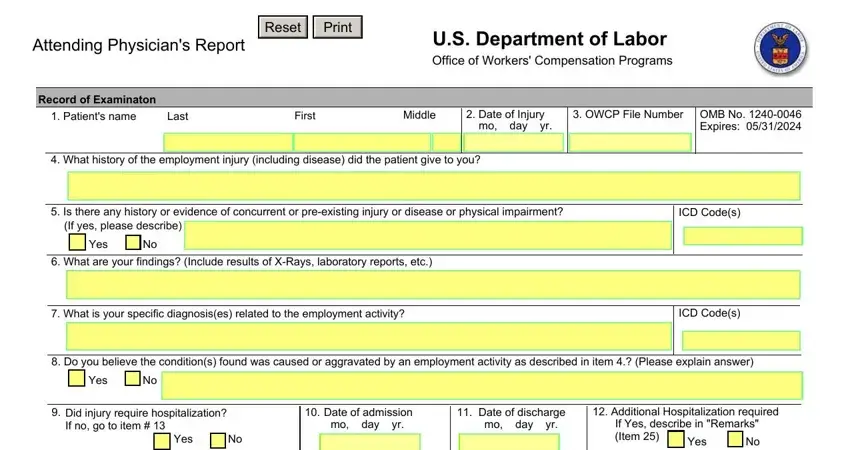
If you want to complete the ca 20 form PDF, provide the information for all of the segments:
Write the necessary information in the What treatment did you provide, Date of first examination mo day, Dates of treatment mo day yr, mo day yr, mo day yr, Date of discharge from treatment, mo day yr, Period of total disability From, Period of Partial Disability From, mo day yr, light work, mo day yr, Date employee able to resume, Date employee is able to resume, and work segment.
Inside the field referring to Signature I certify that the, Signature of Physician, Name of Physician, Address, City, State, ZIP, If yes indicate specialty, Date, Tax ID Number, Do you specialize, Yes, If you have a disability and are, and CA Rev, make sure you note some demanded details.
Step 3: Hit the button "Done". The PDF document is available to be transferred. You can easily upload it to your computer or email it.
Step 4: Just be sure to make as many copies of the form as you can to stay away from future problems.
