
Using PDF files online is super easy with our PDF tool. You can fill out dmv dl546 here painlessly. To make our editor better and simpler to work with, we constantly develop new features, with our users' suggestions in mind. To get started on your journey, go through these simple steps:
Step 1: Just press the "Get Form Button" in the top section of this site to see our pdf editor. Here you will find everything that is necessary to fill out your document.
Step 2: After you open the tool, you'll notice the form all set to be filled out. Apart from filling in various blanks, it's also possible to do other actions with the form, that is putting on any words, changing the initial text, adding illustrations or photos, affixing your signature to the PDF, and a lot more.
This form will require specific data to be filled in, hence ensure you take whatever time to type in exactly what is expected:
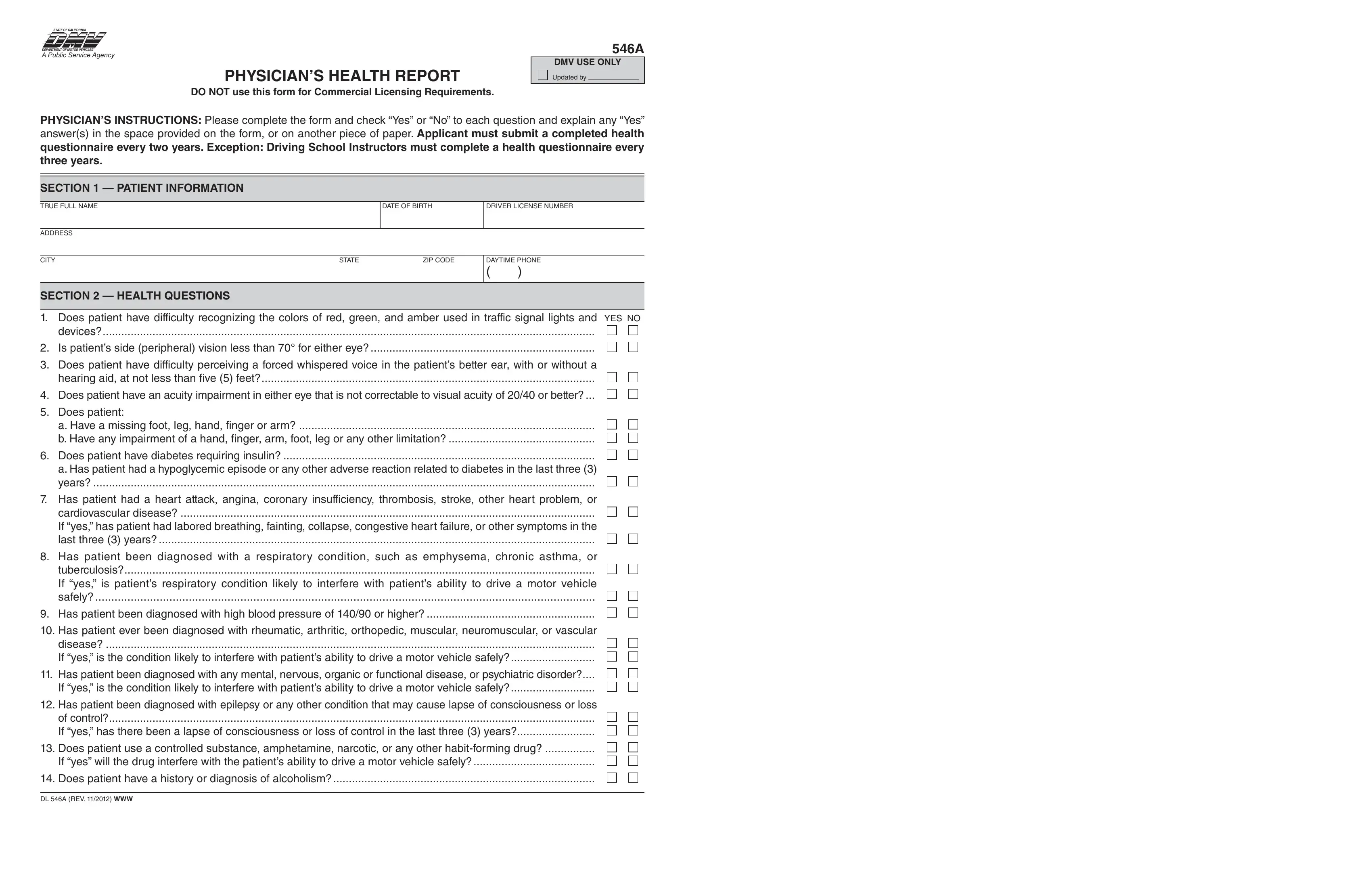
1. Complete your dmv dl546 with a group of essential blank fields. Note all the necessary information and make sure absolutely nothing is omitted!
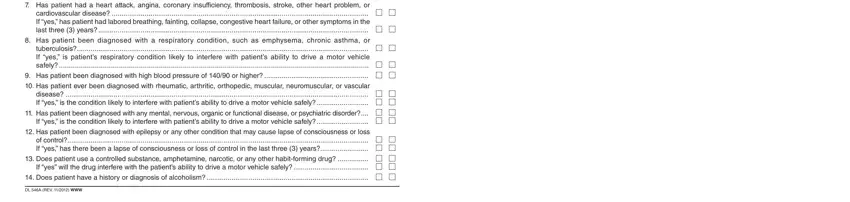
2. Just after the last section is filled out, go on to type in the relevant information in these: has patient had a heart attack, has patient been diagnosed with a, has patient been diagnosed with, has patient ever been diagnosed, has patient been diagnosed with, has patient been diagnosed with, does patient use a controlled, does patient have a history or, and dl a rev WWW.
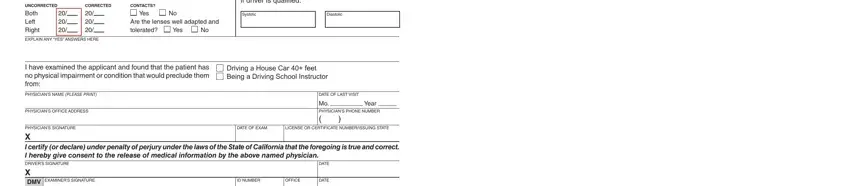
3. The next segment is considered fairly easy, UNCORRECTED both left right, CORRECTED , exPlaiN aNY Yes aNswers here, CONTACTS, Yes, are the lenses well adapted and, Yes, Blood Pressure if consistently mm, systolic, diastolic, i have examined the applicant and, Driving a House Car feet Being a, PhYsiciaNs Name PLEASE PRINT, PhYsiciaNs office address, and date of last visit - all of these blanks must be filled in here.
Be very mindful when filling out systolic and are the lenses well adapted and, since this is where a lot of people make a few mistakes.
Step 3: Before getting to the next stage, double-check that blanks were filled out correctly. Once you confirm that it is correct, click on “Done." Download the dmv dl546 as soon as you join for a 7-day free trial. Immediately get access to the pdf file in your FormsPal account, along with any modifications and changes being automatically preserved! We don't sell or share any details that you type in whenever dealing with forms at our site.