
Should you need to fill out calhr form, there's no need to download any software - just make use of our PDF tool. Our tool is consistently evolving to grant the very best user experience attainable, and that's because of our resolve for constant enhancement and listening closely to comments from users. With a few simple steps, you are able to start your PDF editing:
Step 1: Hit the "Get Form" button above. It will open up our tool so you could start filling out your form.
Step 2: This editor provides you with the ability to work with your PDF form in a range of ways. Improve it by adding any text, adjust what is originally in the file, and include a signature - all readily available!
With regards to the blanks of this precise PDF, here is what you need to know:
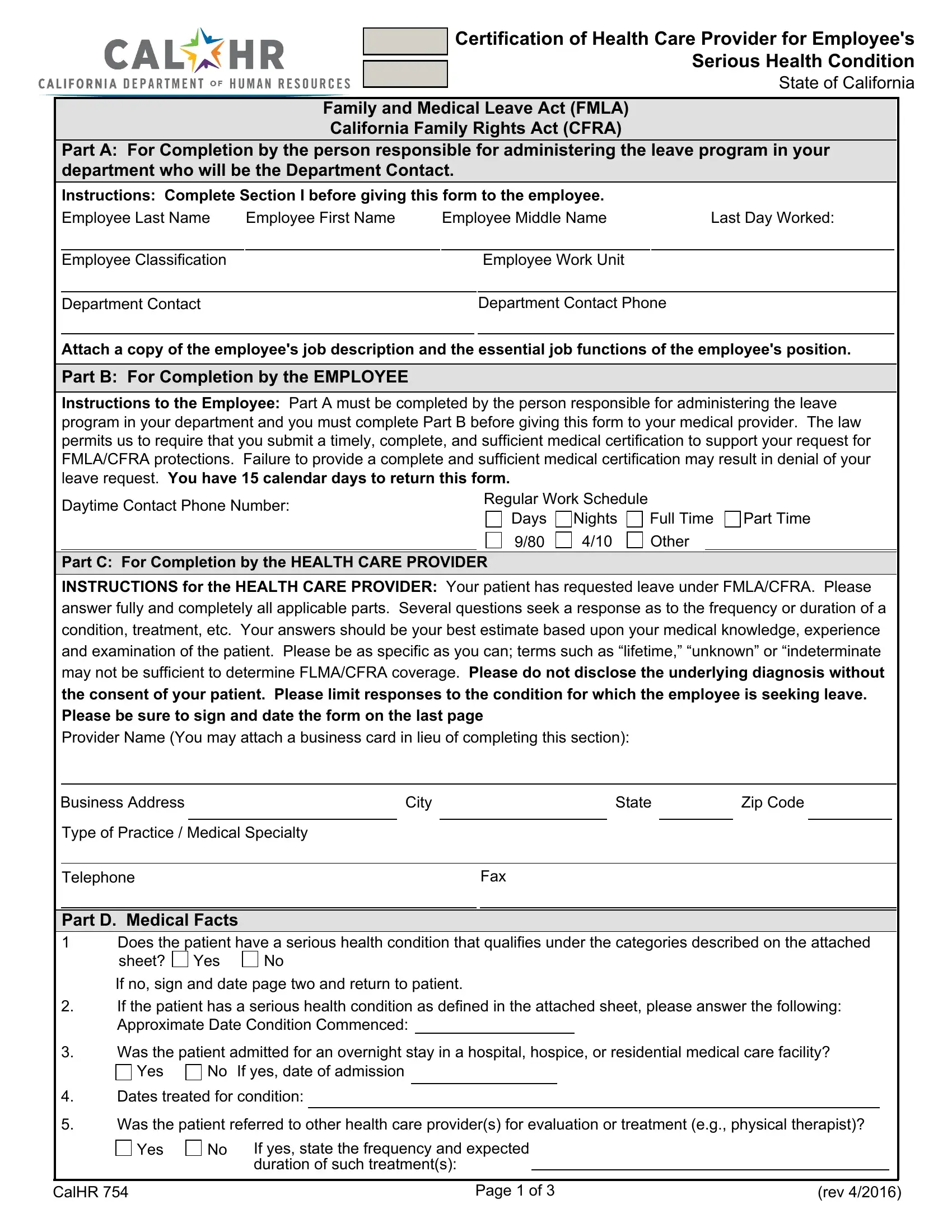
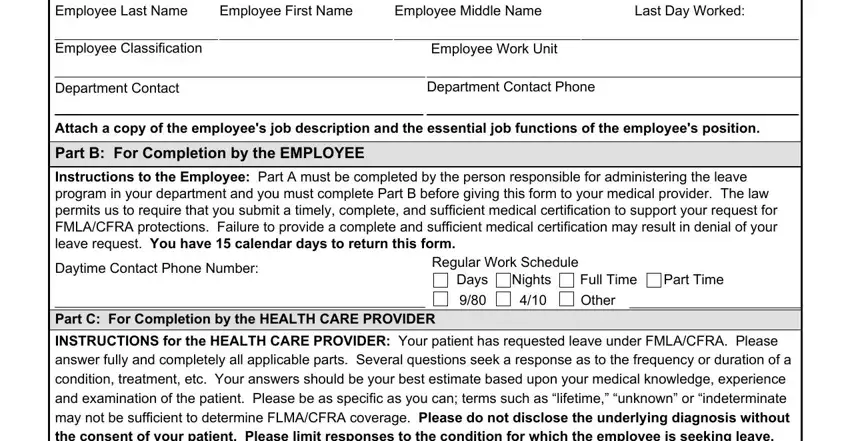
1. The calhr form needs certain details to be entered. Be sure that the next blank fields are complete:
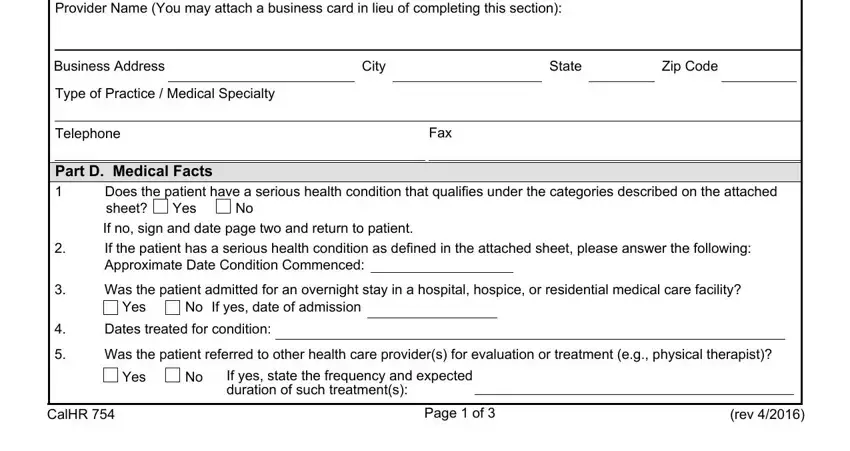
2. After this part is completed, you're ready to put in the essential specifics in INSTRUCTIONS for the HEALTH CARE, Business Address, City, State, Zip Code, Type of Practice Medical Specialty, Telephone, Fax, Part D Medical Facts , Does the patient have a serious, Yes, If no sign and date page two and, If the patient has a serious, Was the patient admitted for an, and Yes so you're able to move forward further.
3. Completing Employee Last Name, Employee First Name, Employee Middle Name, See attached Essential Job, Is the employee unable to perform, Yes, If yes identify the job functions, Can the patient perform modified, Yes, Part E Amount of Time Needed , Will the employee be incapacitated, Yes, Will the employee need to attend, and Yes is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
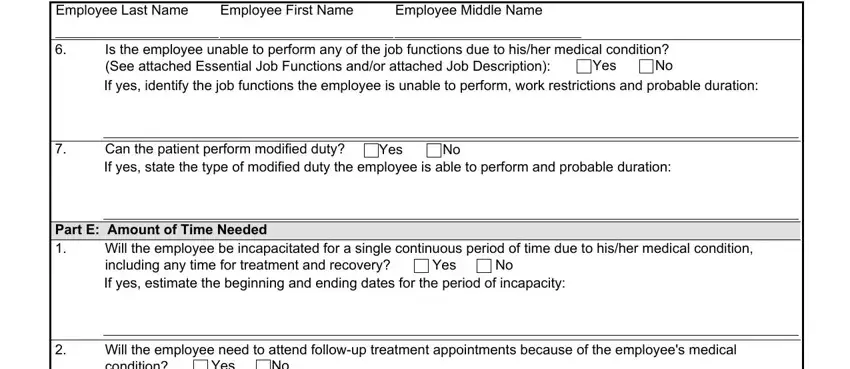
As to Is the employee unable to perform and See attached Essential Job, be certain that you double-check them here. These are definitely the most significant fields in this PDF.
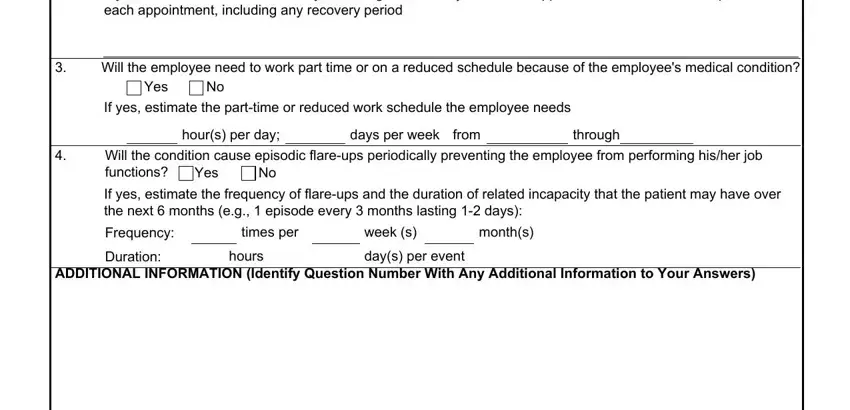
4. The next section needs your attention in the subsequent parts: If yes estimate the schedule if, Will the employee need to work, Yes, If yes estimate the parttime or, hours per day, days per week, from, through, Will the condition cause episodic, Yes, If yes estimate the frequency of, Frequency, Duration, times per, and week s. Remember to fill out all required details to move onward.
5. The form needs to be completed by filling in this segment. Further you'll see an extensive set of blank fields that need to be filled in with correct information for your document usage to be accomplished: Printed Name of Health Care, Health Care Provider Signature, Date, CalHR , Page of , and rev .

Step 3: Always make sure that the information is accurate and simply click "Done" to finish the task. After setting up afree trial account here, it will be possible to download calhr form or email it immediately. The document will also be readily available via your personal account page with all your changes. Here at FormsPal.com, we endeavor to guarantee that all your information is maintained private.