The State of California, through its Department of Human Resources, offers government employees a range of benefits, including the Premier Vision Plan (PVP), formalized via the CalHR 774 form. This document, fundamental for enrollment, alteration, or cancellation of vision insurance coverage, demands careful completion, generally in ink or typewritten to ensure clarity. Intended for those opting in or altering their choices in vision coverage, it facilitates the authorization of deductions from salaries to fund the insurance. Each section caters to a specific need: personal employee details, dependent information for those adding or removing individuals from their plan, and the election section where the employee's intent regarding enrollment is recorded. Moreover, it goes beyond mere procedural steps by emphasizing its privacy terms and the impact of decisions on plan eligibility and duration. Unique identifiers like Social Security numbers are prerequisites, serving dual roles in identification for the State Controller’s Office and for processing by the vision plan vendor. The backdrop of this system is a legal and regulatory framework designed to protect personal information while ensuring the proper administration of benefits. Understanding the terms outlined on both sides of the form is crucial, as it outlines the obligations concerning enrollment duration, dependent eligibility, and the handling of personal data. The CalHR 774 form, revised in February 2013, underscores the state's commitment to offering its employees comprehensive vision care in a structured and secure manner.
| Question | Answer |
|---|---|
| Form Name | Calhr 774 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | cal hr 774 form, calhr form 744, forms calhr 774, alhr 774 |
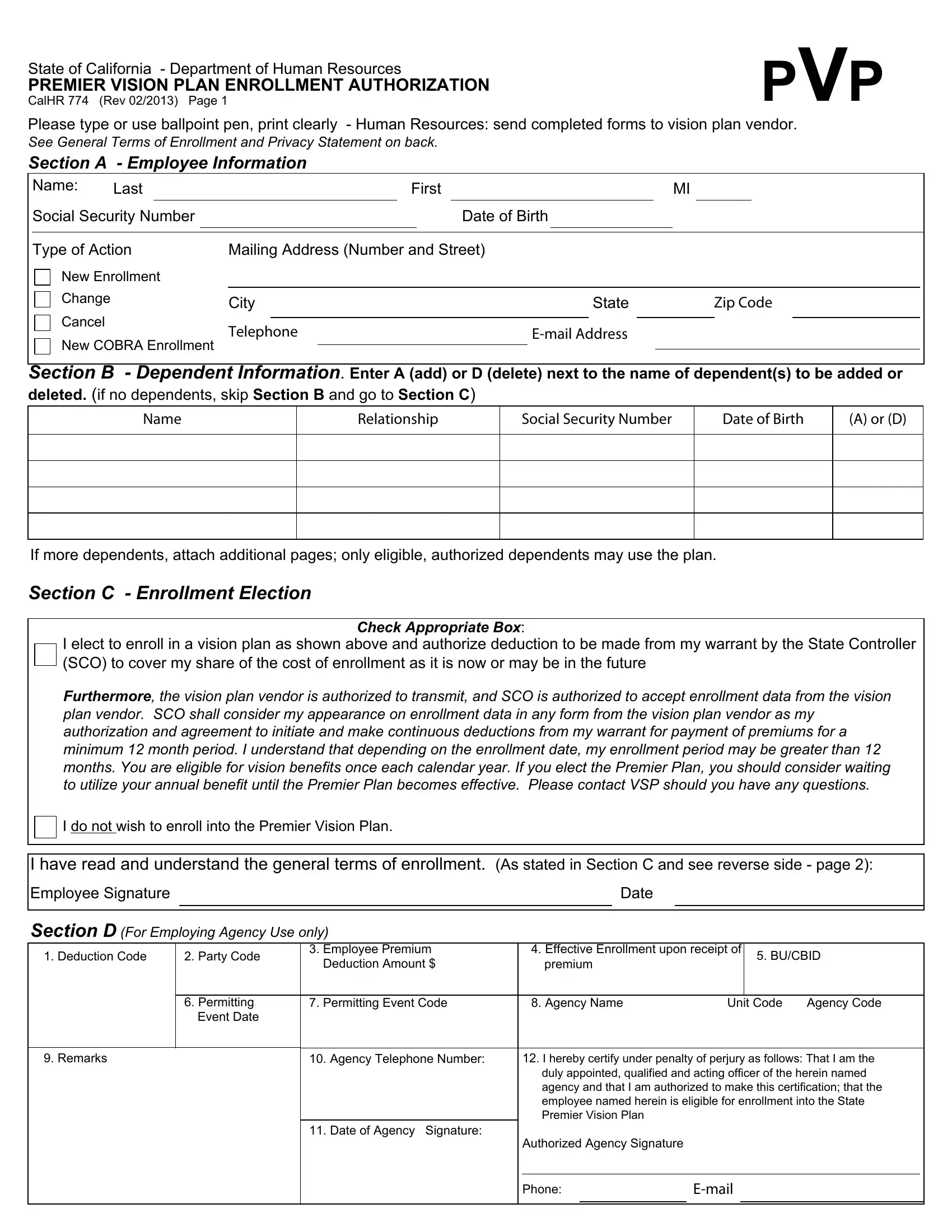
State of California - Department of Human Resources
PREMIER VISION PLAN ENROLLMENT AUTHORIZATION
CalHR 774 (Rev 02/2013) Page 1
PVP
Please type or use ballpoint pen, print clearly - Human Resources: send completed forms to vision plan vendor.
See General Terms of Enrollment and Privacy Statement on back.
Section A - Employee Information
|
Name: |
Last |
|
|
|
First |
|
MI |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Social Security Number |
|
|
|
|
|
Date of Birth |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Action |
Mailing Address (Number and Street) |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
New Enrollment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Change |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
State |
|
|
Zip Code |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
Cancel |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
New COBRA Enrollment |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Section B - Dependent Information. Enter A (add) or D (delete) next to the name of dependent(s) to be added or
deleted. (if no dependents, skip Section B and go to Section C)
Name
Relationship
Social Security Number
Date of Birth
(A) or (D)
If more dependents, attach additional pages; only eligible, authorized dependents may use the plan.
Section C - Enrollment Election
Check Appropriate Box:
I elect to enroll in a vision plan as shown above and authorize deduction to be made from my warrant by the State Controller (SCO) to cover my share of the cost of enrollment as it is now or may be in the future
Furthermore, the vision plan vendor is authorized to transmit, and SCO is authorized to accept enrollment data from the vision plan vendor. SCO shall consider my appearance on enrollment data in any form from the vision plan vendor as my authorization and agreement to initiate and make continuous deductions from my warrant for payment of premiums for a minimum 12 month period. I understand that depending on the enrollment date, my enrollment period may be greater than 12 months. You are eligible for vision benefits once each calendar year. If you elect the Premier Plan, you should consider waiting to utilize your annual benefit until the Premier Plan becomes effective. Please contact VSP should you have any questions.
I do not wish to enroll into the Premier Vision Plan.
I have read and understand the general terms of enrollment. (As stated in Section C and see reverse side - page 2):
Employee Signature |
|
Date |
|
|
|
Section D (For Employing Agency Use only)
1. Deduction Code |
2. Party Code |
3. Employee Premium |
|
4. Effective Enrollment upon receipt of |
5. BU/CBID |
|||||
|
|
Deduction Amount $ |
|
premium |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. Permitting |
7. Permitting Event Code |
|
8. Agency Name |
Unit Code |
Agency Code |
||||
|
Event Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
9. Remarks |
|
10. Agency Telephone Number: |
|
12. I hereby certify under penalty of perjury as follows: That I am the |
||||||
|
|
|
|
duly appointed, qualified and acting officer of the herein named |
||||||
|
|
|
|
agency and that I am authorized to make this certification; that the |
||||||
|
|
|
|
employee named herein is eligible for enrollment into the State |
||||||
|
|
|
|
Premier Vision Plan |
|
|
|
|
|
|
|
|
11. Date of Agency Signature: |
|
|
|
|
|
|
|
|
|
|
|
|
Authorized Agency Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State of California - Department of Human Resources
PREMIER VISION PLAN ENROLLMENT AUTHORIZATION
CalHR 774 (Rev 02/2013) Page 2
PRIVACY NOTICE:
The Information Practices Act of 1977 (Civil Code Section 1798.17) and the Federal Privacy Act (Public Law
Information requested on this form is used by the vision plan vendor and the vision insurance company for the purposes of identification and coverage processing.
It is mandatory to furnish all information requested on this form except for employee's gender and marital status, which may be furnished on a voluntary basis and are used by the vision insurance company for statistical and actuarial purposes. Failure to provide the mandatory information may result in the vision insurance enrollment action not being processed or being processed incorrectly.
The State Controller's requires employee's social security number and name for identification purposes. Legal references authorizing maintenance of this information include Government Code Sections 1151 and 1153, Sections 6011 and 6051 of the Internal Revenue Code, and Regulation 4, Section 404.1256, Code of Federal Regulations under Section 218, Title II of the Social Security Act.
Information provided on the form will be forwarded to the vision insurance company providing coverage for the employee. Copies of the Premier Vision Plan Enrollment Authorization are maintained in confidential files of the State Controller's Office for five years. Employees have the right of access to copies of their Premier Vision Plan Enrollment Authorizations upon request. Send requests to: State Controller's Office, Personnel/Payroll Operations Bureau, P.O. Box 942850, Sacramento, California,
General Terms of Enrollment - Please read carefully:
Employees enrolling into this program will be restricted to maintaining enrollment for a minimum period of 12 months. Length of enrollment may be greater depending upon when you enroll into the plan. A plan year runs from January 1 of any year through December 31 of the same calendar year. Employees enrolling into this program will be restricted to maintaining their enrollment for the balance of the plan year in which they enroll and must maintain enrollment for 12 months in the following plan year unless a permitting event occurs to change their enrollment. Permitting event policy is established by the plan administrator, the California Department of Human Resources.
Only eligible dependents may be enrolled into this plan with the employee. Should you as the eligible employee enroll ineligible dependents, or otherwise maintain ineligible dependents on your plan, you may be held liable for the cost of any and all claims for services rendered. An ineligible dependent is any person you have enrolled onto your vision benefits plan or otherwise maintained on your vision benefits and is not considered an eligible dependent under the enrollment rules of the Department of Human Resources. Should you have questions related to enrollment under this program, you may contact the California Department of Human Resources at: (916)