
You are able to fill in ca dmv driver medical questionnaire form without difficulty in our online PDF tool. We at FormsPal are dedicated to providing you with the absolute best experience with our tool by consistently adding new functions and enhancements. Our editor is now a lot more user-friendly as the result of the newest updates! At this point, editing PDF forms is easier and faster than before. This is what you would need to do to begin:
Step 1: Just hit the "Get Form Button" at the top of this page to access our pdf editing tool. There you'll find all that is needed to work with your document.
Step 2: This editor helps you work with almost all PDF files in a range of ways. Change it by writing customized text, correct original content, and add a signature - all close at hand!
As for the blank fields of this precise PDF, here's what you want to do:
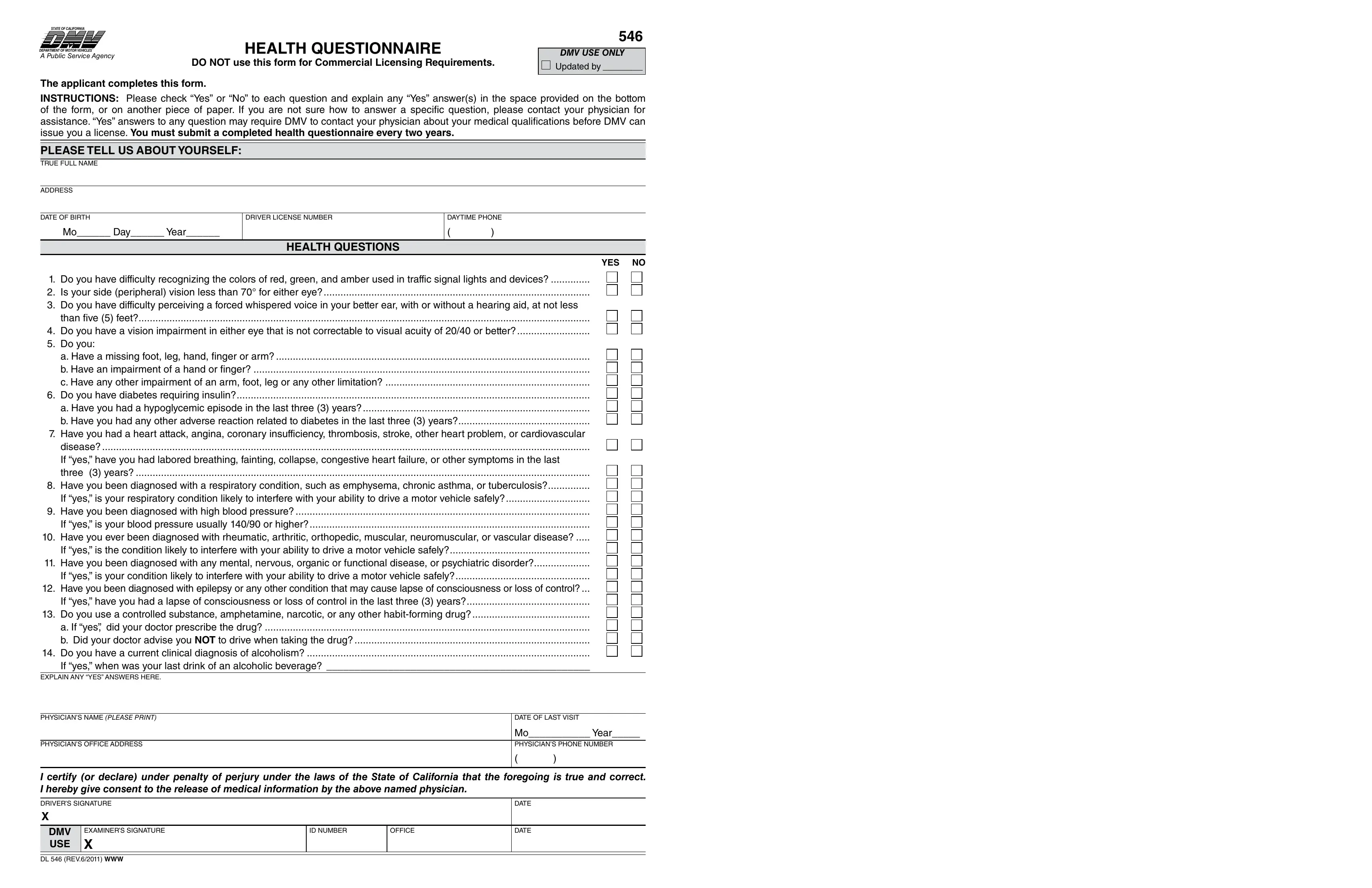
1. Fill out the ca dmv driver medical questionnaire form with a number of major blank fields. Get all of the important information and make sure there is nothing overlooked!
2. Right after this selection of blank fields is filled out, go to type in the relevant details in all these: than ive feet do you have a, Physicians name PLEASE PRINT, Physicians office address, date of last visit, mo year Physicians Phone number, I certify or declare under penalty, drivers siGnature X, DMV USE, examiners siGnature X, dl rev WWW, id number, office, date, and date.
Regarding office and than ive feet do you have a, make sure that you get them right in this current part. These two are considered the key fields in this page.
Step 3: When you have looked over the information you filled in, just click "Done" to complete your form at FormsPal. After starting a7-day free trial account with us, it will be possible to download ca dmv driver medical questionnaire form or send it through email immediately. The PDF document will also be available via your personal account with all of your edits. FormsPal is dedicated to the confidentiality of our users; we make certain that all personal data coming through our system stays protected.