





California Form Ad 9 can be filled out online with ease. Just try FormsPal PDF editor to perform the job fast. The editor is constantly improved by us, getting awesome functions and turning out to be better. To get the ball rolling, consider these easy steps:
Step 1: Open the form inside our tool by clicking the "Get Form Button" at the top of this page.
Step 2: With the help of this advanced PDF editor, you're able to do more than just fill in blank form fields. Try all of the features and make your forms look great with custom textual content added, or adjust the file's original input to perfection - all that comes with the capability to add any images and sign it off.
It is actually an easy task to fill out the pdf using out helpful guide! Here is what you must do:
1. Begin filling out the California Form Ad 9 with a selection of major blanks. Gather all the required information and make certain nothing is left out!
2. Given that the last array of fields is finished, you have to insert the required details in NAME OF CDSS DISTRICT OFFICE OR, and Please fill out as completely as so you can proceed further.
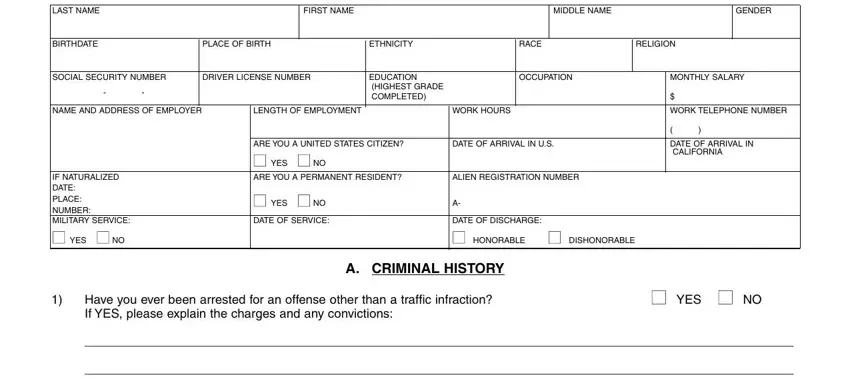
3. Within this step, look at LAST NAME, FIRST NAME, MIDDLE NAME, GENDER, I FIRST PETITIONERS INFORMATION, BIRTHDATE, PLACE OF BIRTH, ETHNICITY, RACE, RELIGION, SOCIAL SECURITY NUMBER, DRIVER LICENSE NUMBER, EDUCATION HIGHEST GRADE COMPLETED, OCCUPATION, and MONTHLY SALARY. Each one of these are required to be filled in with highest focus on detail.
4. Filling in Are you currently on probation or, YES NO, Have you ever been investigated, YES NO, Have you ever been reported for, YES NO, B FORMER MARRIAGESREGISTERED, and WHERE is key in the next part - make certain that you spend some time and be mindful with every single empty field!
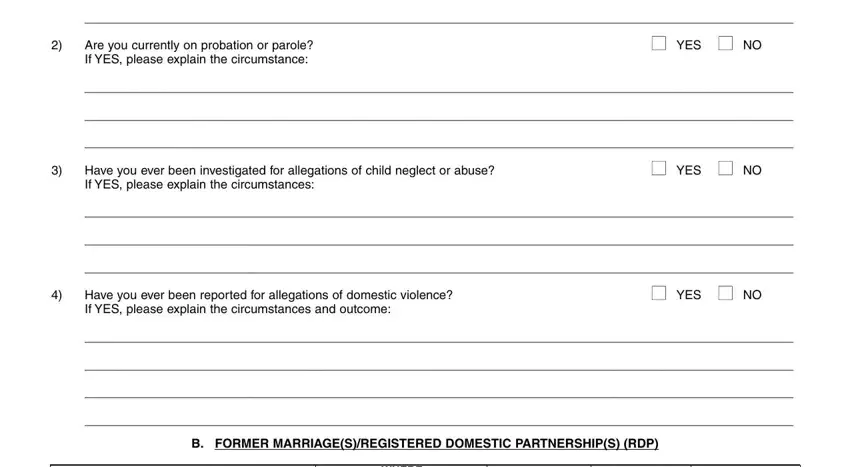
Always be very careful while completing YES NO and WHERE, as this is the section where most users make mistakes.
5. Now, the following last section is what you should wrap up before closing the PDF. The blanks at this stage are the following: Issued in CountyState, Date Place, AD , and PAGE OF .

Step 3: As soon as you have reread the information in the fields, simply click "Done" to conclude your document generation. Get hold of the California Form Ad 9 when you join for a free trial. Instantly gain access to the form from your FormsPal account page, with any edits and adjustments conveniently preserved! FormsPal provides risk-free form editing without data record-keeping or distributing. Rest assured that your data is in good hands with us!