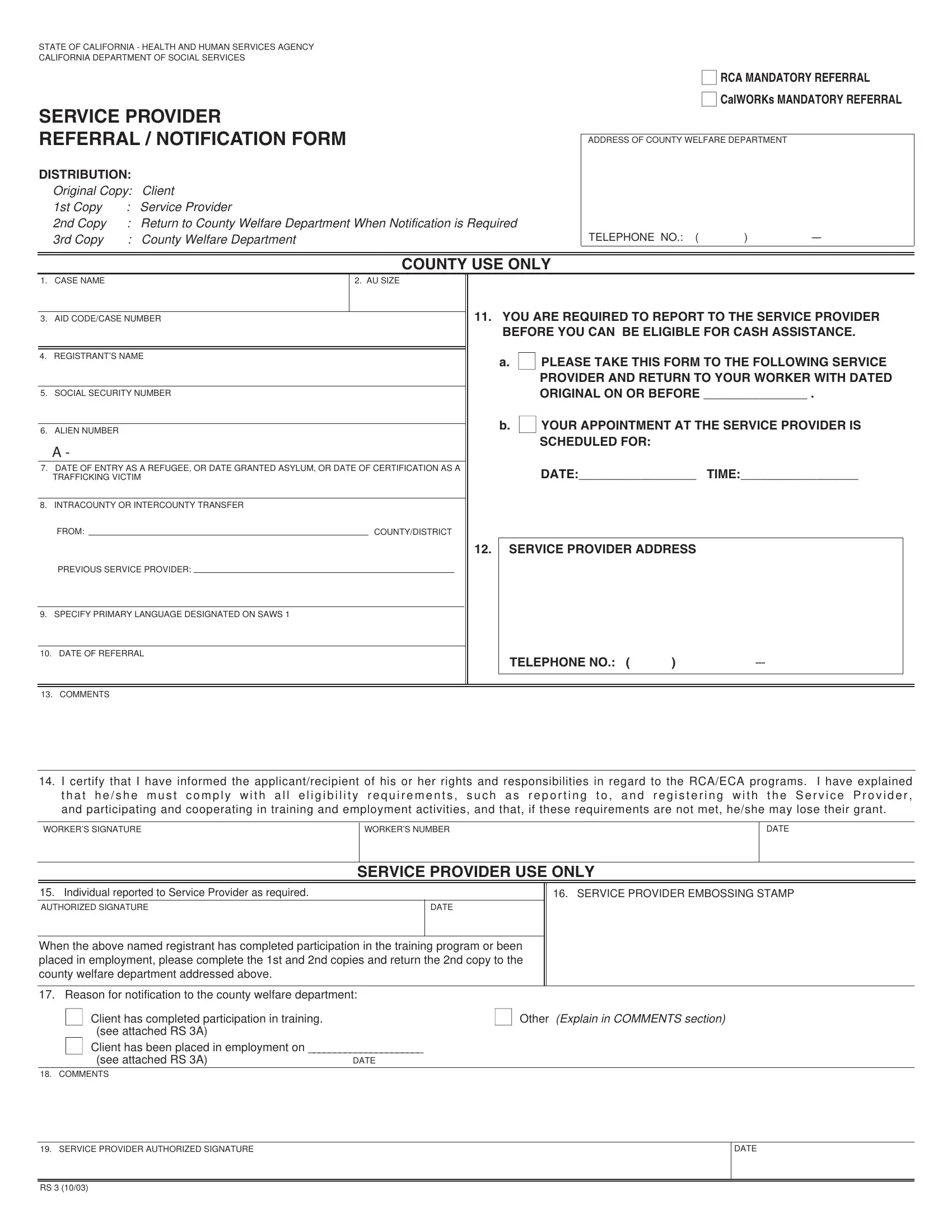
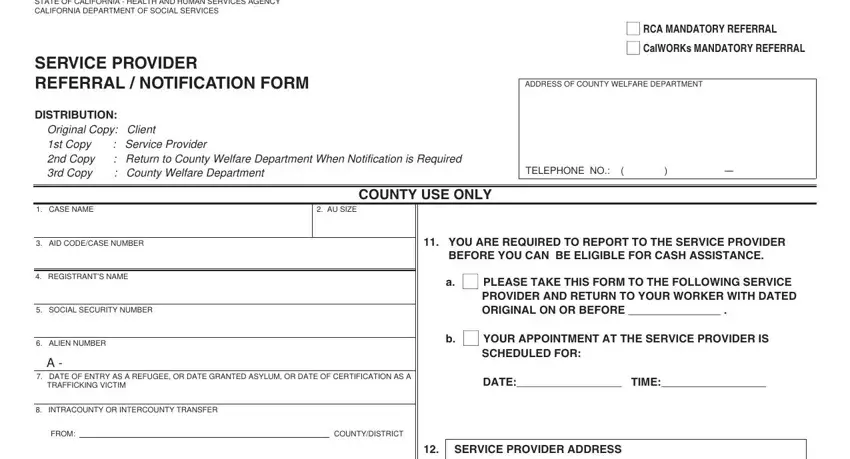
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES
■ RCA MANDATORY REFERRAL
■ CALWORKS MANDATORY REFERRAL
SERVICE PROVIDER
REFERRAL / NOTIFICATION FORM
DISTRIBUTION:
Original Copy: |
Client |
1st Copy |
: |
Service Provider |
2nd Copy |
: |
Return to County Welfare Department When Notification is Required |
3rd Copy |
: |
County Welfare Department |
ADDRESS OF COUNTY WELFARE DEPARTMENT
|
|
|
|
|
COUNTY USE ONLY |
|
|
|
1. |
CASE NAME |
2. AU SIZE |
|
|
|
|
|
|
|
|
|
|
|
|
11. YOU ARE REQUIRED TO REPORT TO THE SERVICE PROVIDER |
3. |
AID CODE/CASE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
BEFORE YOU CAN BE ELIGIBLE FOR CASH ASSISTANCE. |
|
|
|
|
|
|
A. ■ PLEASE TAKE THIS FORM TO THE FOLLOWING SERVICE |
|
|
|
|
|
|
4. |
REGISTRANT’S NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROVIDER AND RETURN TO YOUR WORKER WITH DATED |
|
|
|
|
|
|
|
|
ORIGINAL ON OR BEFORE _______________ . |
5. |
SOCIAL SECURITY NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
B. ■ YOUR APPOINTMENT AT THE SERVICE PROVIDER IS |
6. |
ALIEN NUMBER |
|
|
|
|
|
|
|
|
|
|
|
A - |
|
|
|
|
SCHEDULED FOR: |
|
|
|
|
|
|
|
|
|
|
|
7. |
DATE OF ENTRY AS A REFUGEE, OR DATE GRANTED ASYLUM, OR DATE OF CERTIFICATION AS A |
|
DATE:_________________ |
TIME:_________________ |
|
TRAFFICKING VICTIM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. INTRACOUNTY OR INTERCOUNTY TRANSFER |
|
|
|
|
|
|
|
|
|
FROM: |
|
|
|
COUNTY/DISTRICT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. |
SERVICE PROVIDER ADDRESS |
|
|
|
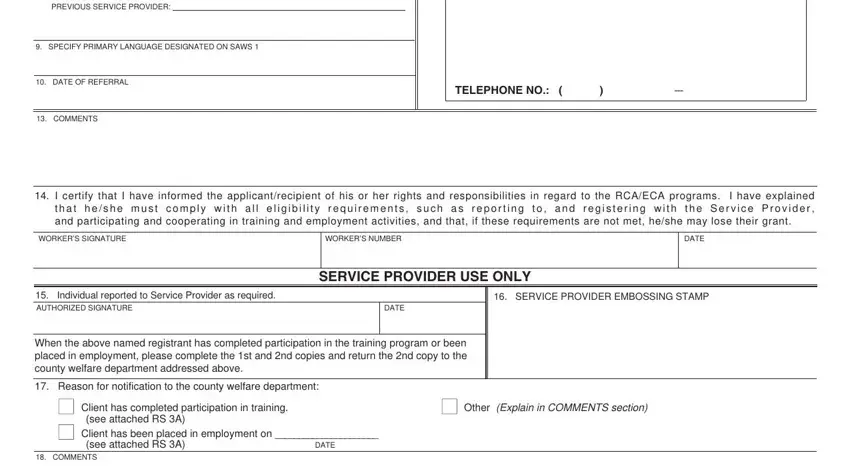
PREVIOUS SERVICE PROVIDER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. SPECIFY PRIMARY LANGUAGE DESIGNATED ON SAWS 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. |
DATE OF REFERRAL |
|
|
|
|
TELEPHONE NO.: ( |
) |
--- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. |
COMMENTS |
|
|
|
|
|
|
|
|
14. I certify that I have informed the applicant/recipient of his or her rights and responsibilities in regard to the RCA/ECA programs. I have explained t h a t h e / s h e m u s t c o m p l y w i t h a l l e l i g i b i l i t y r e q u i r e m e n t s , s u c h a s r e p o r t i n g t o , a n d r e g i s t e r i n g w i t h t h e S e r v i c e P r o v i d e r , and participating and cooperating in training and employment activities, and that, if these requirements are not met, he/she may lose their grant.
|
SERVICE PROVIDER USE ONLY |
|
|
|
|
15. Individual reported to Service Provider as required. |
|
|
16. SERVICE PROVIDER EMBOSSING STAMP |
AUTHORIZED SIGNATURE |
|
DATE |
|
|
|
|
When the above named registrant has completed participation in the training program or been placed in employment, please complete the 1st and 2nd copies and return the 2nd copy to the county welfare department addressed above.
17. Reason for notification to the county welfare department:
■ Client has completed participation in training. |
■ Other (Explain in COMMENTS section) |
■ |
(see attached RS 3A) |
|
Client has been placed in employment on ______________________ |
|
(see attached RS 3A) |
DATE |
18. COMMENTS
19.SERVICE PROVIDER AUTHORIZED SIGNATURE
RS 3 (10/03)
SERVICE PROVIDER REFERRAL FORM
Instructions
County Use Only
1.Case Name --- Enter the refugee’s name: last name, first name, and middle initial.
2.AU Size --- Enter number of persons in the Assistance Unit
3.Aid Code/Case Number --- Enter the two-digit aid identification code for the appropriate public assistance program/Enter the refugee’s case number as assigned by your CWD.
4.Registrant’s Name --- Enter the name of person in the AU who is being referred on a mandatory basis, and required to register with the Service Provider.
5.Social Security Number --- Enter the registrant’s social security number.
6.Alien Number --- Enter the registrant’s alien number.
7.Date of Entry to U.S. or Date Granted Asylum --- Enter the date shown on the registrant’s I-94 form or I-551 form or other appropriate documentation.
8.Intracounty or Intercounty Transfer --- Enter the county (or district, if Los Angeles), and the Service Provider name and address that the registrant is transferring from.
9.Specify primary language designated on SAWS 1.
10.Date of Referral --- Enter the date on which the registrant is referred to the Service Provider.
11a. Check this box and enter the date that the registrant is to return the validated original RS 3 form to the Worker.
11b. If you make an appointment for the registrant to report to the Service Provider, check this box and enter the date and time of the appointment.
12.Service Provider Address --- Enter the address and telephone number of the Service Provider the registrant is being referred to. Enter the Service Provider’s full address including, number, street, city and zip code.
13.Comments --- Self-explanatory.
14.Worker Name and Worker Number --- Enter the name of worker assigned to the case, and the number that your county uses to identify the worker.
Service Provider Use Only
15.Authorized Signature --- This is to be signed by the person authorized to certify that the registrant has reported to the Service Provider for registration.
16.Service Provider Embossing Stamp --- Enter the official certification stamp.
17.Check the appropriate box to indicate why notification is being made.
18.Comments --- Self-explanatory.
19.Service Provider Authorized Signature --- This is to be signed and dated by the person authorized to complete this form.