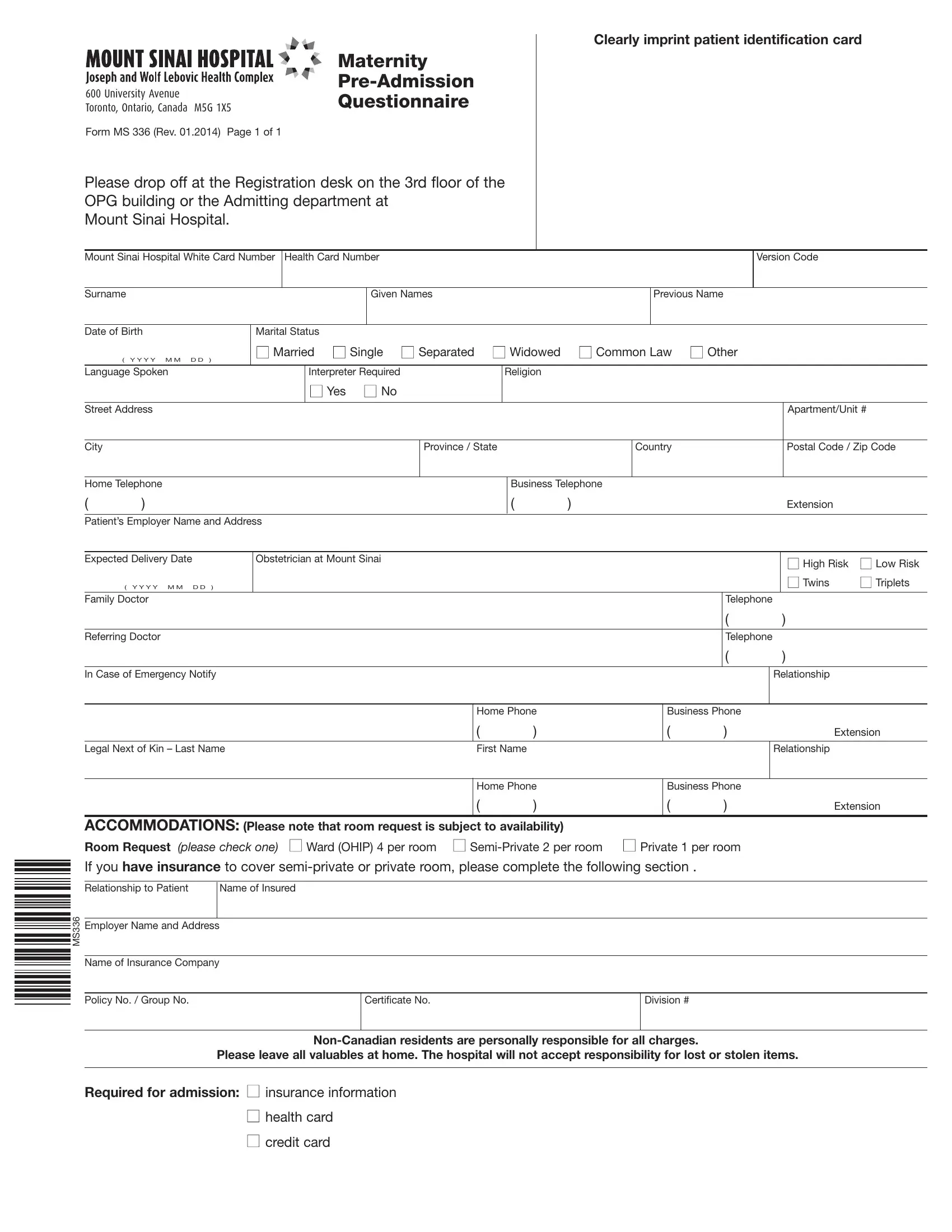
Navigating the journey to motherhood often involves meticulous preparation, especially when it involves hospital pre-admissions for the awaited day. In Canada, one crucial step in this preparation is filling out the Canada MS 336 form, a comprehensive document designed to streamline the maternity pre-admission process at medical facilities, including the notable Mount Sinai Hospital in Toronto, Ontario. As of its latest revision in January 2014, the form encapsulates essential information ranging from patient identification, such as the Mount Sinai Hospital White Card Number and Health Card Number, to more personal details like marital status, language preferences, and the necessity for an interpreter. It even dives into specifics of the expected delivery - delineating between high or low-risk pregnancies and the possibility of multiples. Furthermore, it covers emergency contacts and legal next of kin, ensuring the hospital is well-prepared to handle any situation that may arise. Additionally, accommodation preferences are addressed, offering options from ward to private rooms, subject to availability and insurance coverage, underlining the need for patients to manage expectations regarding their stay. Importantly, the form also highlights the responsibility of non-Canadian residents for all charges and reminds patients to leave valuables at home, as the hospital cannot guarantee their safety. Lastly, it specifies the essential items for admission: insurance information, health card, and credit card, ensuring patients are fully prepared for their hospital visit.
| Question | Answer |
|---|---|
| Form Name | Canada Form Ms 336 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 2014, OPG, M5G, Sinai |
|
|
|
|
|
|
|
Maternity |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
600 University Avenue |
||||||||
Questionnaire |
||||||||
Toronto, Ontario, Canada M5G 1X5 |
||||||||
|
||||||||
Form MS 336 (Rev. 01.2014) Page 1 of 1 |
|
|||||||
Please drop off at the Registration desk on the 3rd floor of the OPG building or the Admitting department at
Mount Sinai Hospital.
Clearly imprint patient identification card
Mount Sinai Hospital White Card Number
Health Card Number
Version Code
Surname
Given Names
Previous Name
Date of Birth |
Marital Status |
|
■ Married ■ Single ■ Separated |
■ Widowed ■ Common Law ■ Other |
||
( Y Y Y Y M M |
D D ) |
|
|
|
Language Spoken |
|
Interpreter Required |
|
Religion |
|
|
■ Yes ■ No |
|
|
|
|
|
|
|
Street Address
City
|
|
|
Apartment/Unit # |
Province / State |
|
Country |
Postal Code / Zip Code |
|
|||
|
|
|
|
Home Telephone
()
Business Telephone
( |
) |
Extension |
Patient’s Employer Name and Address
Expected Delivery Date |
|
Obstetrician at Mount Sinai |
■ High Risk |
■ Low Risk |
|
|
|
|
|
||
( Y Y Y Y M M D D |
) |
|
|
■ Twins |
■ Triplets |
|
|
|
|
||
Family Doctor |
|
|
Telephone |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
Referring Doctor |
|
|
Telephone |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
In Case of Emergency Notify
Relationship
|
Home Phone |
Business Phone |
|
||
|
( |
) |
( |
) |
Extension |
|
|
|
|
|
|
Legal Next of Kin – Last Name |
First Name |
|
|
|
Relationship |
|
|
|
|
|
|
Home Phone
()
Business Phone
( |
) |
Extension |
ACCOMMODATIONS: (Please note that room request is subject to availability)
Room Request (please check one) ■ Ward (OHIP) 4 per room ■
If you have insurance to cover
MS336
Relationship to Patient |
Name of Insured |
|
|
Employer Name and Address
Name of Insurance Company
Policy No. / Group No. |
Certificate No. |
Division # |
|
|
|
Please leave all valuables at home. The hospital will not accept responsibility for lost or stolen items.
Required for admission: ■ insurance information
■health card
■credit card