Navigating the processes involved in securing reimbursement for services and entitlements can be complex, particularly for veterans seeking to utilize their benefits. The Canvet Claim Center form serves as a crucial tool in this endeavor, offering a structured means for Veterans Affairs Canada clients to claim these expenses. This comprehensive document is designed to capture all relevant information across several sections, including personal identification details, the nature and amount of the claim, and specifics regarding travel for assessments not related to schooling. It necessitates the submission of original bills, receipts, and other supporting documents to avoid denial. Moreover, the form outlines the requirement for claims to be filed within a year of incurring the expenditure, emphasizes the individual's understanding of and agreement with the claims guidelines, and insists on the authenticity and completeness of the provided information. The protection of personal information is governed by the Privacy Act, ensuring confidentiality and security of the data provided. It also underscores the responsibility of claimants to include all necessary documentation, such as original receipts and educational institution documentation where applicable, to facilitate a smooth and timely reimbursement process. Failure to adhere to these guidelines not only delays payment but possibly results in denial, underlining the importance of thoroughness in completing the Canvet Claim Center form.
| Question | Answer |
|---|---|
| Form Name | Canvet Claim Center Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 5th, 3K3, online canveter com, V8V |
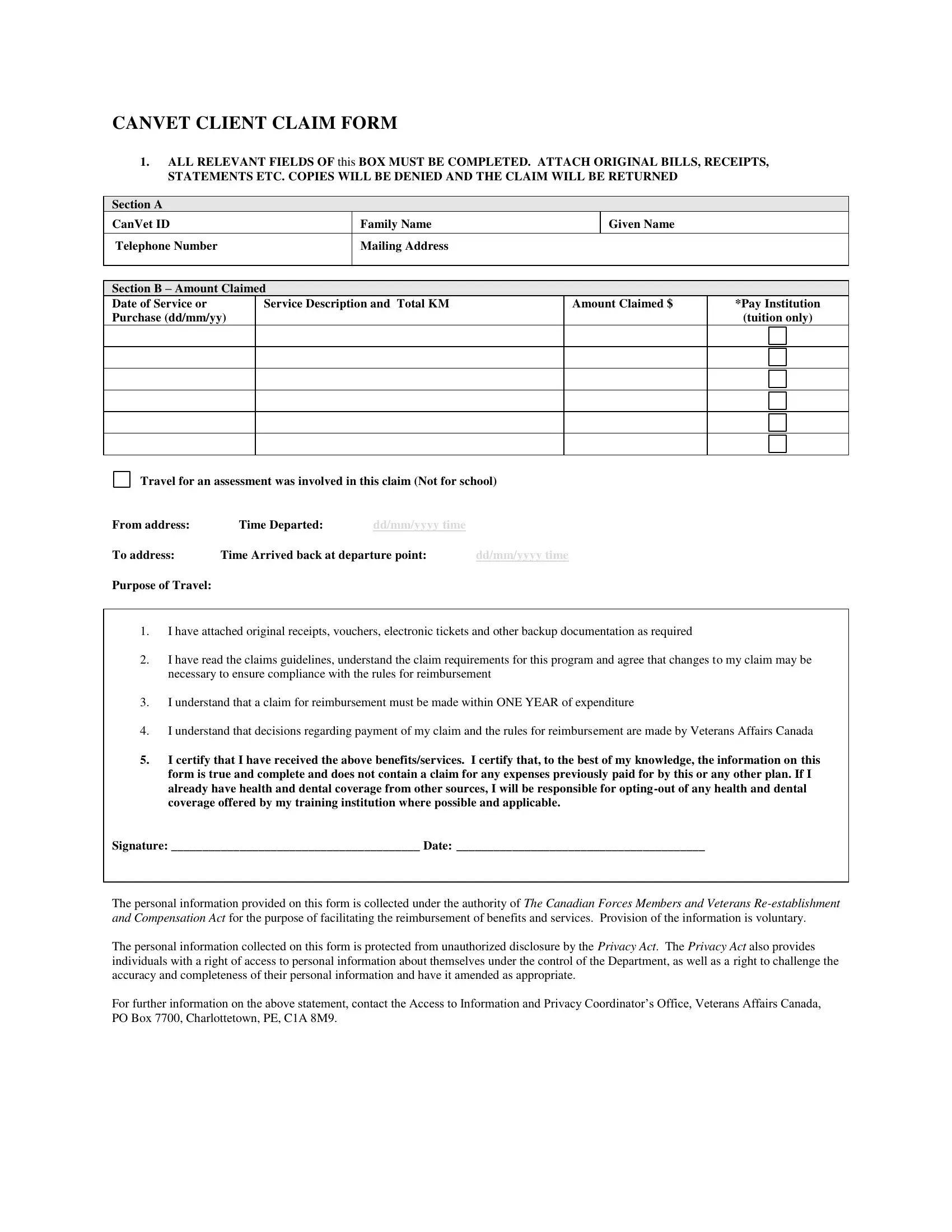
CANVET CLIENT CLAIM FORM
1.ALL RELEVANT FIELDS OF this BOX MUST BE COMPLETED. ATTACH ORIGINAL BILLS, RECEIPTS,
STATEMENTS ETC. COPIES WILL BE DENIED AND THE CLAIM WILL BE RETURNED
Section A
CanVet ID |
|
Family Name |
|
Given Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone Number |
|
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Section B – Amount Claimed |
|
|
|
|
|
||
Date of Service or |
Service Description and Total KM |
Amount Claimed $ |
*Pay Institution |
|||||
Purchase (dd/mm/yy) |
|
|
|
|
(tuition only) |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Travel for an assessment was involved in this claim (Not for school)
From address: |
Time Departed: |
dd/mm/yyyy time |
|
To address: |
Time Arrived back at departure point: |
dd/mm/yyyy time |
|
Purpose of Travel: |
|
|
|
1.I have attached original receipts, vouchers, electronic tickets and other backup documentation as required
2.I have read the claims guidelines, understand the claim requirements for this program and agree that changes to my claim may be necessary to ensure compliance with the rules for reimbursement
3.I understand that a claim for reimbursement must be made within ONE YEAR of expenditure
4.I understand that decisions regarding payment of my claim and the rules for reimbursement are made by Veterans Affairs Canada
5.I certify that I have received the above benefits/services. I certify that, to the best of my knowledge, the information on this form is true and complete and does not contain a claim for any expenses previously paid for by this or any other plan. If I already have health and dental coverage from other sources, I will be responsible for
Signature: ________________________________________ Date: ________________________________________
The personal information provided on this form is collected under the authority of The Canadian Forces Members and Veterans
The personal information collected on this form is protected from unauthorized disclosure by the Privacy Act. The Privacy Act also provides individuals with a right of access to personal information about themselves under the control of the Department, as well as a right to challenge the accuracy and completeness of their personal information and have it amended as appropriate.
For further information on the above statement, contact the Access to Information and Privacy Coordinator’s Office, Veterans Affairs Canada, PO Box 7700, Charlottetown, PE, C1A 8M9.
In order to obtain prompt payment of your claim, did you…
Complete and sign your claim form?
Include original receipts (NO Photocopies OR Faxes)?
Staple all receipts and documentation to the claim?
Include documentation from the educational institution indicating that the following items are
“required”: books, tools, safety clothing, software, equipment, etc (see documentation)?
List mileage by day or week showing each day that was traveled?
Provide a rationale if travel occurred during a weekend or statutory holiday?
Verify that you have the most recent copy of your Individual Vocational Rehabilitation Plan (IVRP)?
If you do not, please contact your VAC Case Manager.
Payment of this claim does not indicate that all future claims for these items or services will be approved.
Claims for reimbursement must be made in writing within one year after the day on which the
expenditure was incurred. Claims submitted after that date will be declined.
When Completed, Please Mail Your Claim Form to
CanVet VR Services
Client Claim Processing Centre
5th Floor, 915 Fort Street
Victoria, BC
V8V 3K3
Missing or incorrect information results in unavoidable delays in claims payment.
For questions view our website at WWW.CANVETSERVICES.COM.
Decisions regarding payment of your claim and the rules for reimbursement are made by Veterans
Affairs Canada.