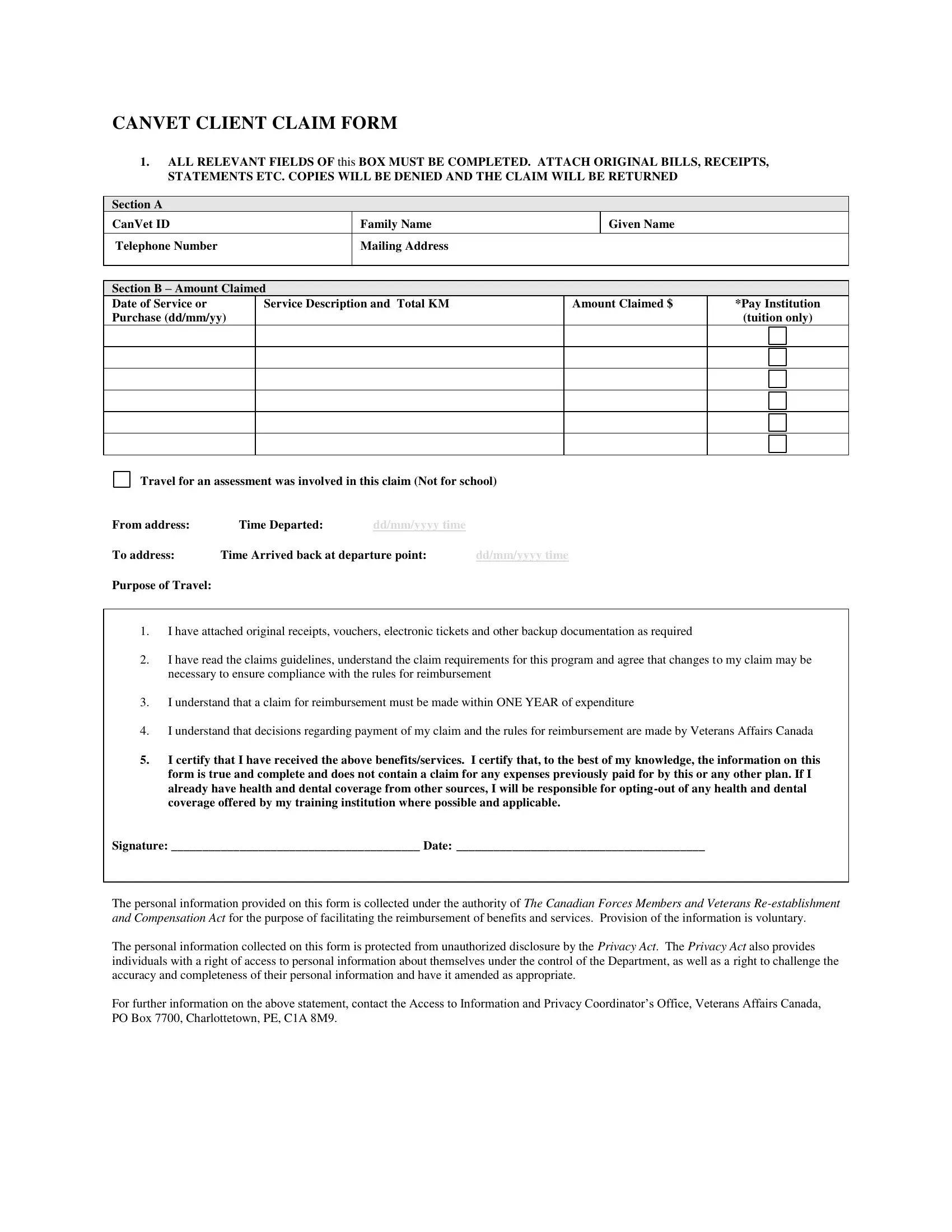
Navigating the processes involved in securing reimbursement for services and entitlements can be complex, particularly for veterans seeking to utilize their benefits. The Canvet Claim Center form serves as a crucial tool in this endeavor, offering a structured means for Veterans Affairs Canada clients to claim these expenses. This comprehensive document is designed to capture all relevant information across several sections, including personal identification details, the nature and amount of the claim, and specifics regarding travel for assessments not related to schooling. It necessitates the submission of original bills, receipts, and other supporting documents to avoid denial. Moreover, the form outlines the requirement for claims to be filed within a year of incurring the expenditure, emphasizes the individual's understanding of and agreement with the claims guidelines, and insists on the authenticity and completeness of the provided information. The protection of personal information is governed by the Privacy Act, ensuring confidentiality and security of the data provided. It also underscores the responsibility of claimants to include all necessary documentation, such as original receipts and educational institution documentation where applicable, to facilitate a smooth and timely reimbursement process. Failure to adhere to these guidelines not only delays payment but possibly results in denial, underlining the importance of thoroughness in completing the Canvet Claim Center form.
| Question | Answer |
|---|---|
| Form Name | Canvet Claim Center Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 5th, 3K3, online canveter com, V8V |