The Chemical Control Order Registration Form is a comprehensive document designed to facilitate the regulation and management of chemicals by various entities. It requires applicants to provide detailed information about their company or identity, including the type of chemicals to be handled and their Chemical Abstract Service (CAS) number. This form is segmented into sections that cover a wide array of essential data such as the applicant's category, which includes importers, distributors, users, transporters of chemicals, waste transporters, treaters, and disposers. Additionally, it seeks specifics on business and storage facility addresses, contact information, and legal registration details like business and SEC registration numbers. An understanding of annual chemical requirements, environmental compliance status, and attachments such as business permits and chemical management plans is also requested. The form not only aims at gathering current operational data but also ensures adherence to environmental standards through certifications and verifications, underscoring the importance of accurate and truthful submissions to potentially influence the application's outcome. Furthermore, the inclusion of quarterly reporting forms emphasizes ongoing compliance and monitoring, illustrating a dynamic approach to chemical management and environmental protection.
| Question | Answer |
|---|---|
| Form Name | Cco Online Application Form |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | cco form, CAS, cco application, form cco |
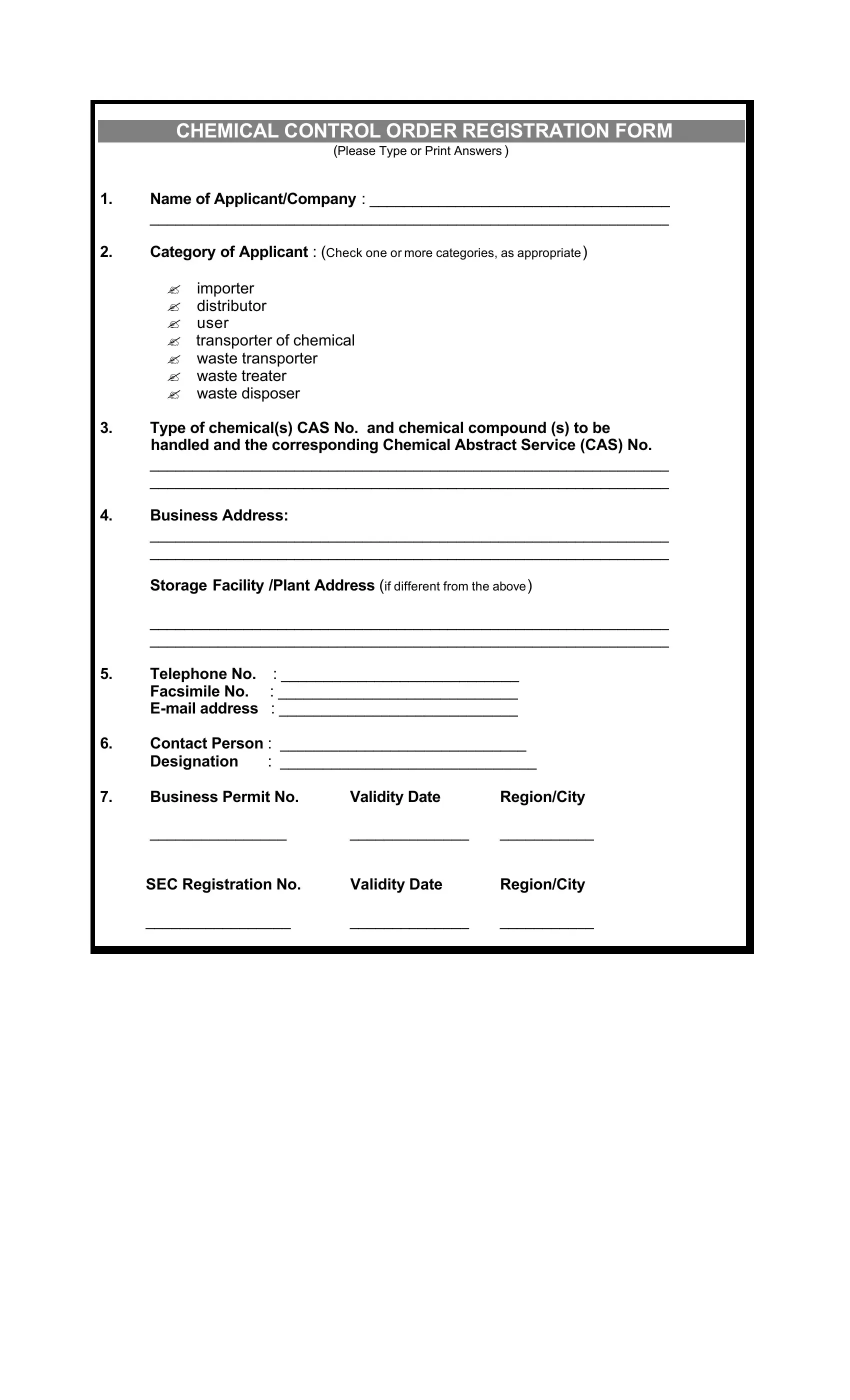
CHEMICAL CONTROL ORDER REGISTRATION FORM
(Please Type or Print Answers )
1.Name of Applicant/Company : ___________________________________
_____________________________________________________________
2.Category of Applicant : (Check one or more categories, as appropriate)
?importer
?distributor
?user
?transporter of chemical
?waste transporter
?waste treater
?waste disposer
3.Type of chemical(s) CAS No. and chemical compound (s) to be handled and the corresponding Chemical Abstract Service (CAS) No.
_____________________________________________________________
_____________________________________________________________
4.Business Address:
_____________________________________________________________
_____________________________________________________________
Storage Facility /Plant Address (if different from the above)
_____________________________________________________________
_____________________________________________________________
5.Telephone No. : ____________________________
Facsimile No. : ____________________________
6.Contact Person : _____________________________
Designation : ______________________________
7. |
Business Permit No. |
Validity Date |
Region/City |
|
________________ |
______________ |
___________ |
|
SEC Registration No. |
Validity Date |
Region/City |
|
_________________ |
______________ |
___________ |
|
|
|
|
|
|
|
|
8.Annual Chemical(s) Requirement (kg or MT) ______________________
____________________________________________________________
9.Status of Compliance to Environmental Permit
|
|
Date of issuance/ |
Region/City |
|
|
validity date |
|
ECC No. _______________ |
__________ |
____________ |
|
Permit to Operate Number |
|
|
|
air |
_______________ |
__________ |
____________ |
water |
______________ |
__________ |
____________ |
10.Attachments (Please attach a photocopy of the following)
Business Permit
SEC Registration
Chemical Management Plan
Copy of Environmental Permits
11.Certification:
I certify that the data and information hereto stated in this form and attachments are true and correct. I understand that any false or misleading statements may result in permanent denial of my/my company’s application or cancellation of my/my company’s registration.
Date of application : _________________________________
Signature of Authorized Person : _________________________________
Printed Name |
: _________________________________ |
Title/Designation |
: ________________________________ |
_____________________________________________________________________
DO NOT WRITE IN THIS SPACE
Chemical(s) Applied For : ________________________________
Endorsement and Inspection Report Date:____________________
Information checked by : ________________________________
Fee : ________________ Official Receipt No. ___________
First Verification Date : _________________
Second Verification Date : _________________
“CCO QUARTERLY REPORT FORM”
(Please Type or Print Answers )
For the period ______,20___.”
1.Name of Company:
_____________________________________________________________________
_____________________________________________________________________
2.Business Address:
_____________________________________________________________________
_____________________________________________________________________
Telephone No.: ______________________ Fax No:__________________________
Storage Facility Address : _______________________________________________
_____________________________________________________________________
_____________________________________________________________________
Telephone No.: _______________________ Fax No.: _________________________
3.License Number : _____________________Sector Code:_____________________
4.CHEMICAL SPECIFIC INFORMATION: (Please attach
(a)“Common Name/ IUPAC/CAS Index Name: ____________________________.”
________________________________________________________________
(b)Cas No. _______________________
(c)Trade Name :______________________________________________________
“ For Importers”
Requested
Import
Clearance
Number
Date of Arrival
Quantity* Received
Shipping
Vessel
Country of
Origin
Country
of
Manufacture
*attach Bill of Lading
“For Transporters”
(d)Total Quantity Transported: ______________________________________________
Date of Transport |
: |
_______________________________________________ |
Quantity Transported |
: |
_______________________________________________ |
Source of material/address |
: _____________________________________________ |
|
Destination |
: _______________________________________________ |
|
Date of Transport |
: _______________________________________________ |
|
Quantity Transported |
: _______________________________________________ |
|
Source of material/address |
: _____________________________________________ |
|
Destination |
: _______________________________________________ |
|
“For Distributors” |
|
|
(e) Total quantity Distributed |
: ______________________________________________ |
|
Name of client |
:_________________________________________________ |
|
License No. |
: ________________________________________________ |
|
Quantity |
: ________________________________________________ |
|
Date of Distribution |
: ________________________________________________ |
|
Name of transporter |
: ________________________________________________ |
|
License No. |
: ________________________________________________ |
|
Date of Transport |
: ________________________________________________ |
|
Name of Client |
: ________________________________________________ |
|
License No. |
: ________________________________________________ |
|
Quantity |
: ________________________________________________ |
|
Date of Distribution |
: ________________________________________________ |
|
Name of transporter |
: ________________________________________________ |
|
License No. |
: ________________________________________________ |
|
Date of Transport |
: ________________________________________________ |
|
Name of client |
: ________________________________________________ |
|
License No. |
: ________________________________________________ |
|
Quantity |
: ________________________________________________ |
|
Date of Distribution |
: ________________________________________________ |
|
Name of transporter |
: ________________________________________________ |
|
License No. |
: ________________________________________________ |
|
Date of Transport |
: ________________________________________________ |
|
“For
(f)Total quantity purchased from distributors: _________________________________
Name of distributor |
: ____________________________________________________ |
License No. |
: ____________________________________________________ |
Quantity |
: ____________________________________________________ |
Date of Purchase |
“ |
|
Name of Transporter: _____________________________________________________________ |
|||
|
License Number. |
: _____________________________________________________________ |
||
|
Date of Transport |
: _____________________________________________________________ |
||
|
Name of Distributor |
: _____________________________________________________________ |
||
|
License Number |
: _____________________________________________________________ |
||
|
Quantity |
: _____________________________________________________________ |
||
|
Date of Purchase |
: _____________________________________________________________ |
||
|
Name of Transporter : _____________________________________________________________ |
|||
|
License Number |
: _____________________________________________________________ |
||
|
Date of Transport |
: _____________________________________________________________ |
||
“For users and manufacturers” |
|
|||
5. |
Use and Production : |
|
||
|
Total Production Quantity : ______________________________________________________ |
|||
|
Quantity Used |
|
: ______________________________________________________ |
|
|
(a) |
enclosed process |
:_________________________________________________(kgs) |
|
(b)controlled release process : ______________________________________________(kgs)
(c) |
Open process |
: _________________________________________________(kgs) |
6.Quantity of waste chemical generated : _____________________________________________
7.Quantity of stock inventory : ______________________________________________________
8.Chemical Handling Information
Hazardous wastes Registration No.: _________________________________________________
Hazardous wastes Quarterly Report : Date Submitted _______________Region_______________
Manner of handling hazardous wastes
?Storage
?Treatment
?Treatment/Disposal
CHEMICAL CONTROL ORDER REGISTRATION FORM
9.Chemical Use Reduction Plan :
(attach appropriate information)
?Pollution Prevention Plan
?Chemical Substitute Plan
10.Certification:
“ The undersigned certify that the information provided in this form is true and accurate.”
Printed Name: ______________________________________
Signature: _________________________________________
Designation/Position:_________________________________
Date:______________________________________________