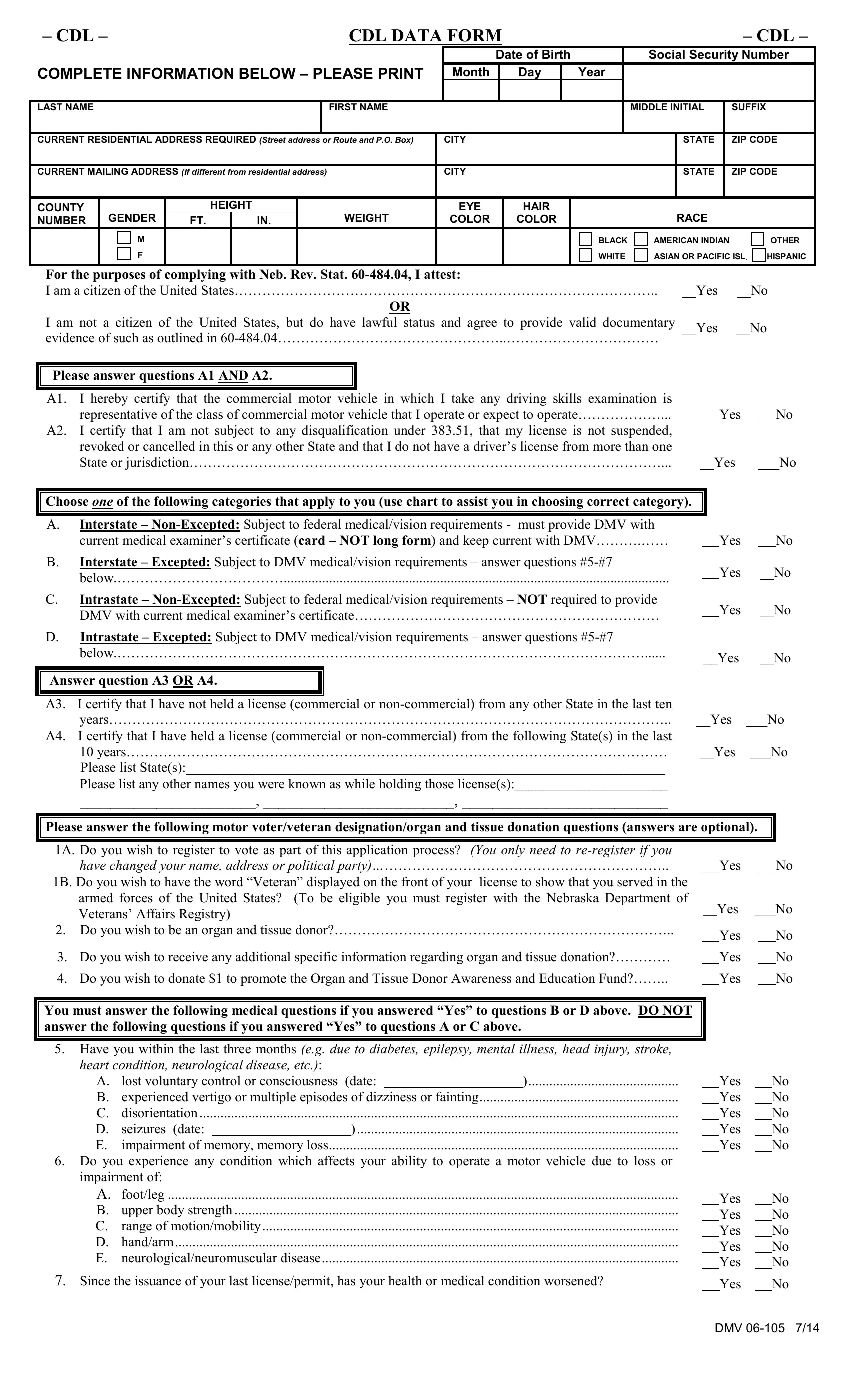
In today’s meticulous documentation era, navigating through official forms can seem like a daunting task, especially when it pertains to regulatory requirements for commercial driving. The CDL Data Form serves as a crucial document for individuals seeking to obtain or renew a Commercial Driver’s License (CDL) in compliance with various regulatory statutes. This comprehensive form requires applicants to provide detailed personal information, including their date of birth, social security number, and residential address, alongside specifics such as height, weight, eye and hair color, and race. It also necessitates declarations regarding the applicant’s citizenship status, adherence to the driving qualification under federal laws, and medical fitness for the role. Furthermore, the form presents a choice between categories that determine the level of medical documentation needed according to the nature of the interstate or intrastate commercial driving the applicant intends to engage in. Prospective CDL holders must certify their history of license possession and declare any name changes to preempt discrepancies in records. It uniquely intertwines voter registration, veteran designation, organ and tissue donation options, and critical health inquiries, reflecting an intersection between legal compliance, civic responsibility, and personal health declaration. By ensuring the accuracy and integrity of the information provided, this form plays a pivotal role in maintaining public safety standards on the road.
| Question | Answer |
|---|---|
| Form Name | Cdl Data Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | nebraska form dmv 06 104, A4, 3RD, A2 |
|
– CDL – |
|
|
|
|
|
CDL DATA FORM |
|
|
|
|
|
– CDL – |
|||||||
|
|
|
|
|
|
|
|
|
|
|
Date of Birth |
|
|
Social Security Number |
||||||
COMPLETE INFORMATION BELOW – PLEASE PRINT |
Month |
|
|
Day |
|
Year |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
|
|
|
|
FIRST NAME |
|
|
|
|
|
|
|
MIDDLE INITIAL |
|
SUFFIX |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
CURRENT RESIDENTIAL ADDRESS REQUIRED (STREET ADDRESS OR ROUTE AND P.O. BOX) |
|
CITY |
|
|
|
|
|
|
|
STATE |
|
ZIP CODE |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
CURRENT MAILING ADDRESS (IF DIFFERENT FROM RESIDENTIAL ADDRESS) |
|
|
CITY |
|
|
|
|
|
|
|
STATE |
|
ZIP CODE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COUNTY |
GENDER |
|
HEIGHT |
|
WEIGHT |
|
EYE |
|
|
HAIR |
|
|
|
RACE |
|
|||||
NUMBER |
FT. |
|
IN. |
|
|
COLOR |
|
|
COLOR |
|
|
|
|
|||||||
|
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
BLACK |
AMERICAN INDIAN |
OTHER |
|||
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
WHITE |
ASIAN OR PACIFIC ISL. HISPANIC |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For the purposes of complying with Neb. Rev. Stat.
I am a citizen of the United States………………………………………………………………………………..
OR
I am not a citizen of the United States, but do have lawful status and agree to provide valid documentary evidence of such as outlined in
__Yes __No
__Yes __No
Please answer questions A1 AND A2.
A1. |
I hereby certify that the commercial motor vehicle in which I take any driving skills examination is |
|
|
|
|
|
|
representative of the class of commercial motor vehicle that I operate or expect to operate………………... |
|
|
Yes |
|
No |
A2. |
I certify that I am not subject to any disqualification under 383.51, that my license is not suspended, |
|
|
|
|
|
|
revoked or cancelled in this or any other State and that I do not have a driver’s license from more than one |
|
|
|
|
|
|
State or jurisdiction…………………………………………………………………………………………... |
__Yes |
___No |
|||
Choose ONE of the following categories that apply to you (use chart to assist you in choosing correct category).
A.Interstate –
B.Interstate – Excepted: Subject to DMV medical/vision requirements – answer questions
C.Intrastate –
D.Intrastate – Excepted: Subject to DMV medical/vision requirements – answer questions
Answer question A3 OR A4.
Yes No
Yes __No
Yes __No
__Yes __No
A3. |
I certify that I have not held a license (commercial or |
|
|
|
years………………………………………………………………………………………………………….. |
__Yes |
___No |
A4. |
I certify that I have held a license (commercial or |
|
|
|
10 years……………………………………………………………………………………………………… |
__Yes |
___No |
|
Please list State(s):_____________________________________________________________________ |
|
|
|
Please list any other names you were known as while holding those license(s):______________________ |
|
|
|
_______________________, _________________________, ___________________________ |
|
|
Please answer the following motor voter/veteran designation/organ and tissue donation questions (answers are optional).
1A. |
Do you wish to register to vote as part of this application process? (You only need to |
|
|
|
|
|
|
have changed your name, address or political party)……………………………………………………….. |
|
Yes |
|
|
No |
1B. Do you wish to have the word “Veteran” displayed on the front of your license to show that you served in the |
|
|
|
|
|
|
|
armed forces of the United States? (To be eligible you must register with the Nebraska Department of |
__Yes |
___No |
|||
|
Veterans’ Affairs Registry) |
|||||
|
|
|
|
|
|
|
2. Do you wish to be an organ and tissue donor?……………………………………………………………….. |
|
Yes |
|
|
No |
|
|
|
|
|
|
||
3. |
Do you wish to receive any additional specific information regarding organ and tissue donation?………… |
|
Yes |
|
|
No |
4. |
Do you wish to donate $1 to promote the Organ and Tissue Donor Awareness and Education Fund?…….. |
|
Yes |
|
|
No |
You must answer the following medical questions if you answered “Yes” to questions B or D above. DO NOT answer the following questions if you answered “Yes” to questions A or C above.
5.Have you within the last three months (e.g. due to diabetes, epilepsy, mental illness, head injury, stroke,
heart condition, neurological disease, etc.): |
|
A. lost voluntary control or consciousness (date: |
) |
B.experienced vertigo or multiple episodes of dizziness or fainting
C.disorientation..................................................................................................................................................................................................
D. seizures (date: |
|
) |
E.impairment of memory, memory loss....................................................................................................
6.Do you experience any condition which affects your ability to operate a motor vehicle due to loss or impairment of:
A.foot/leg ..................................................................................................................................................
B.upper body strength...............................................................................................................................
C.range of motion/mobility.......................................................................................................................
D.hand/arm................................................................................................................................................
E.neurological/neuromuscular disease......................................................................................................
7.Since the issuance of your last license/permit, has your health or medical condition worsened?
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
DMV