 OPERATED
OPERATED OWNED
OWNED OPERATED
OPERATED OWNED
OWNED OPERATED
OPERATEDThis PDF editor enables you to fill in documents. You don't have to perform much to modify watercraft accord application forms. Only stick to the next steps.
Step 1: Click the "Get Form Now" button to start out.
Step 2: At the moment you're on the file editing page. You can edit and add text to the document, highlight specified content, cross or check specific words, insert images, insert a signature on it, delete needless areas, or eliminate them entirely.
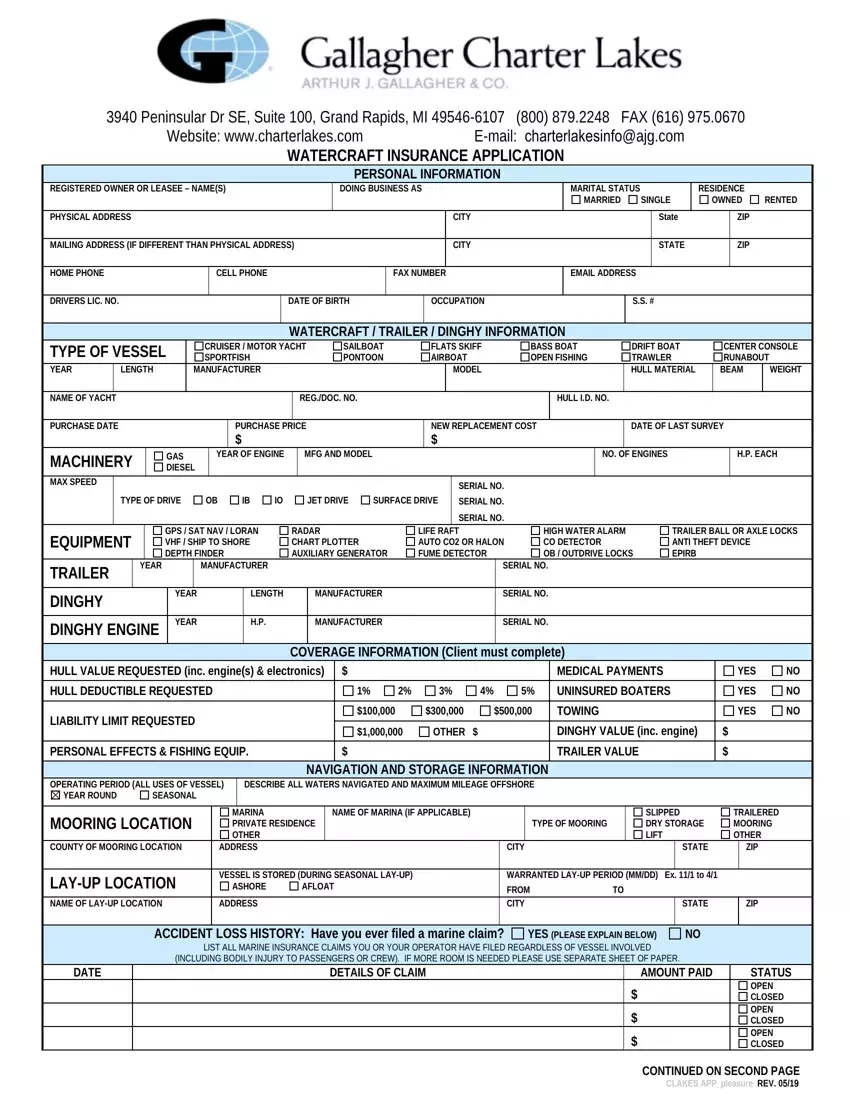
Complete the what is a dte insurance form PDF by providing the information needed for each section.
You need to write down the appropriate information in the GPS SAT NAV LORAN VHF SHIP TO, RADAR CHART PLOTTER AUXILIARY, LIFE RAFT AUTO CO OR HALON FUME, HIGH WATER ALARM CO DETECTOR OB, TRAILER BALL OR AXLE LOCKS ANTI, EQUIPMENT, TRAILER, DINGHY, DINGHY ENGINE, YEAR, MANUFACTURER, YEAR, YEAR, LENGTH, and MANUFACTURER space.
Make sure you provide the crucial information within the LAYUP LOCATION NAME OF LAYUP, ADDRESS, WARRANTED LAYUP PERIOD MMDD Ex to, STATE, ZIP, ACCIDENT LOSS HISTORY Have you, YES PLEASE EXPLAIN BELOW LIST ALL, DATE, DETAILS OF CLAIM, AMOUNT PAID, STATUS OPEN CLOSED OPEN CLOSED, and CONTINUED ON SECOND PAGE CLAKES section.
The IS THIS VESSEL USED FOR CHARTER OR, IF YES PLEASE EXPLAIN, GENERAL INFORMATION, YES, DO YOU TOW SKIERS, YES, IS VESSEL USED FOR RACING, YES, IS VESSEL USED AS A LIVEABOARD NO, YES, PRIMARY RESIDENCE SECONDARY, HAS ANY NAMED INSURED EVER BEEN, YES PLEASE EXPLAIN BELOW, YES, and LIST PREVIOUS VESSELS OWNED OR area will be your place to place the rights and obligations of all sides.
Finalize by reviewing the next sections and filling them in as needed: ADDITIONAL INSURED CERTIFICATE, NAME, ADDRESS STREET CITY STATE ZIP, INTEREST, SPECIAL CONDITIONS COMMENTS, CERT HOLDER, LOSS PAYEE, CERT HOLDER, LOSS PAYEE, CERT HOLDER, LOSS PAYEE, Any person who knowingly and with, HOW DID YOU HEAR ABOUT US, EFFECTIVE DATE OF COVERAGE, and APPLICANT SIGNATURE.
Step 3: Click the "Done" button. Now you may export the PDF form to your gadget. Additionally, it is possible to send it through email.
Step 4: To avoid any specific problems in the future, try to have as a minimum a couple of copies of the file.
