
Using PDF files online is surprisingly easy with our PDF tool. Anyone can fill in sss sickness notification form 2021 here and try out a number of other functions we offer. FormsPal development team is constantly working to enhance the tool and insure that it is much easier for clients with its cutting-edge functions. Make the most of today's modern possibilities, and find a trove of unique experiences! Here is what you'll need to do to get started:
Step 1: Simply press the "Get Form Button" above on this page to see our pdf file editing tool. This way, you will find everything that is required to work with your file.
Step 2: The tool enables you to modify PDF forms in many different ways. Change it by adding customized text, correct what is already in the document, and place in a signature - all within a couple of clicks!
As a way to finalize this PDF document, make certain you type in the right details in every single field:
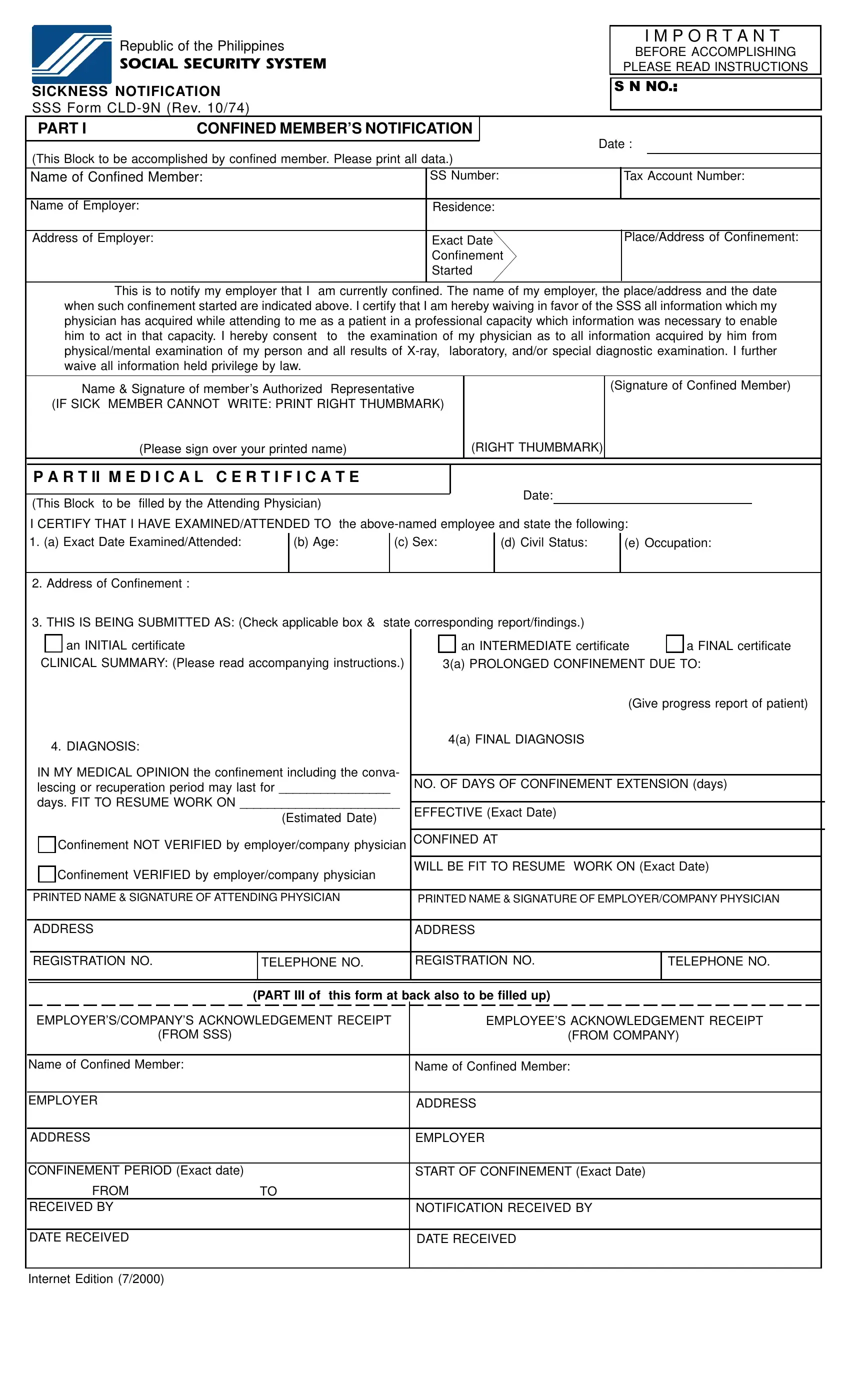
1. It's vital to complete the sss sickness notification form 2021 accurately, hence be mindful when filling out the segments including all these blanks:
2. Just after the previous array of fields is completed, go on to enter the applicable information in these: I CERTIFY THAT I HAVE, d Civil Status, e Occupation, b Age, c Sex, Address of Confinement, THIS IS BEING SUBMITTED AS Check, an INITIAL certificate, an INTERMEDIATE certificate, a FINAL certificate, CLINICAL SUMMARY Please read, a PROLONGED CONFINEMENT DUE TO, Give progress report of patient, DIAGNOSIS, and a FINAL DIAGNOSIS.
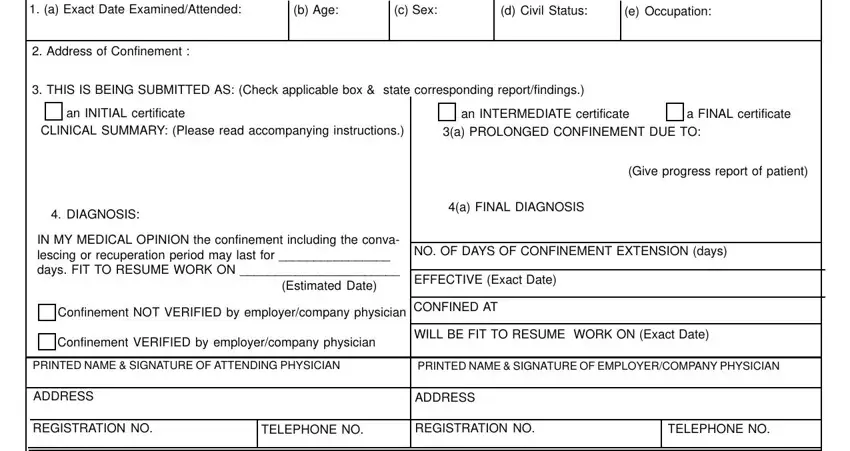
Always be very mindful when filling out c Sex and a FINAL certificate, since this is where many people make errors.
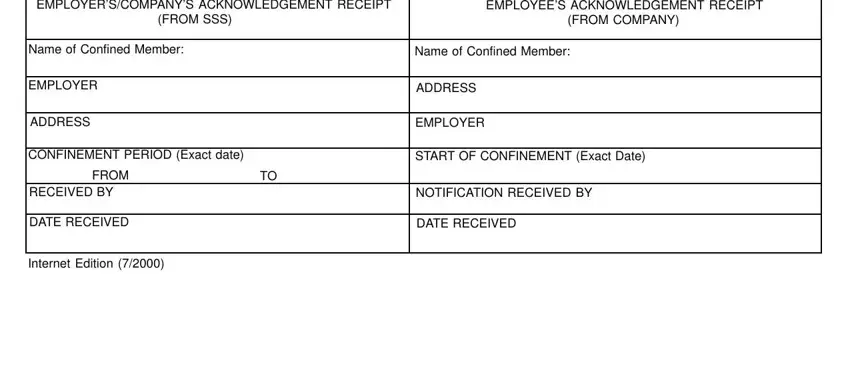
3. Within this part, review EMPLOYERSCOMPANYS ACKNOWLEDGEMENT, EMPLOYEES ACKNOWLEDGEMENT RECEIPT, FROM SSS, FROM COMPANY, Name of Confined Member, Name of Confined Member, EMPLOYER, ADDRESS, ADDRESS, EMPLOYER, CONFINEMENT PERIOD Exact date, START OF CONFINEMENT Exact Date, FROM, RECEIVED BY, and DATE RECEIVED. Each of these need to be taken care of with greatest accuracy.
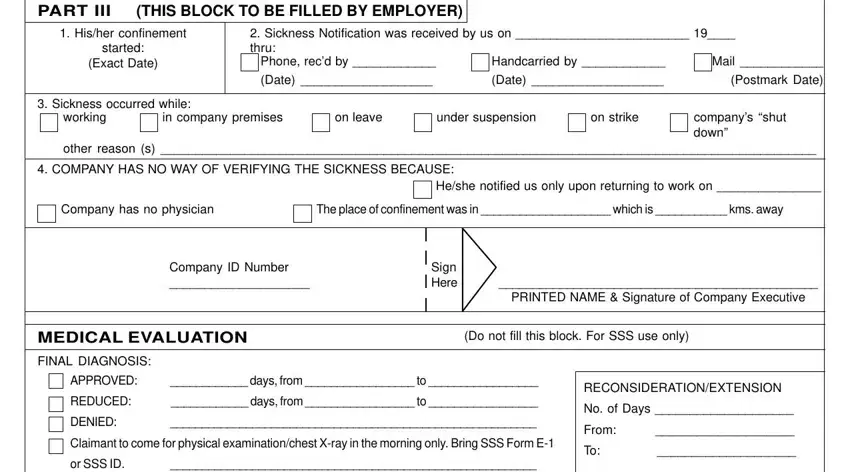
4. To go ahead, the next stage will require completing a few blanks. These comprise of PART III THIS BLOCK TO BE FILLED, Hisher confinement, started, Exact Date, Sickness Notification was, Phone recd by, Handcarried by, Mail, Date, Date, Postmark Date, Sickness occurred while, working, in company premises, and on leave, which you'll find vital to going forward with this process.
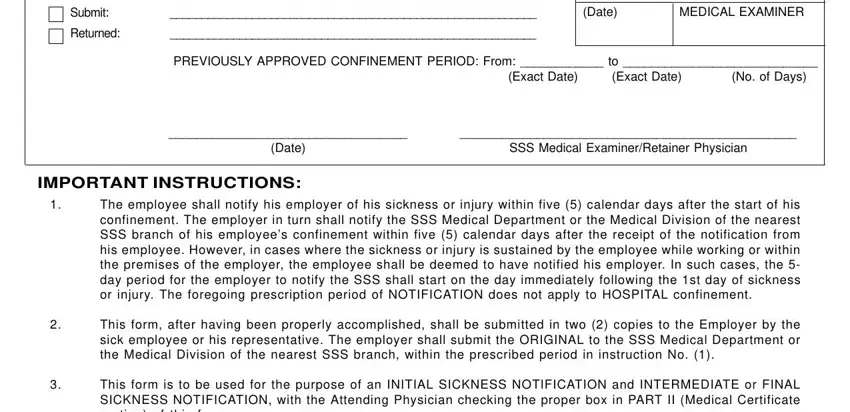
5. The form needs to be concluded by filling in this segment. Below you will find a comprehensive list of fields that need appropriate information in order for your form submission to be complete: Submit, Returned, Date, MEDICAL EXAMINER, PREVIOUSLY APPROVED CONFINEMENT, Exact Date, Exact Date, No of Days, Date, SSS Medical ExaminerRetainer, IMPORTANT INSTRUCTIONS, The employee shall notify his, This form after having been, and This form is to be used for the.
Step 3: Soon after double-checking the fields you've filled out, click "Done" and you're done and dusted! Right after registering a7-day free trial account here, it will be possible to download sss sickness notification form 2021 or email it directly. The document will also be readily accessible through your personal account page with your each and every change. FormsPal provides risk-free document completion without personal data record-keeping or sharing. Rest assured that your information is in good hands with us!