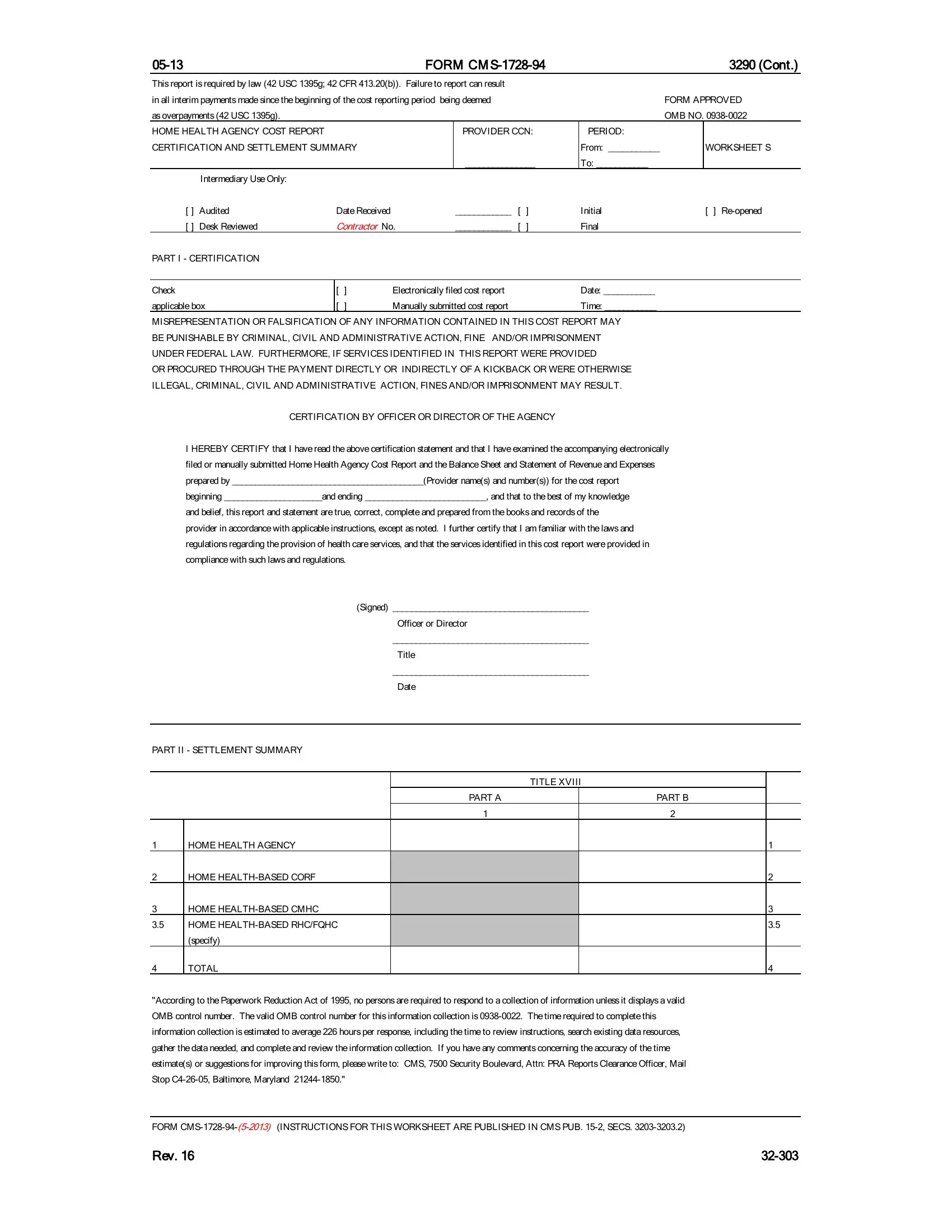
The CMS-1728-94 form, officially known as the Home Health Agency Cost Report, plays a crucial role in the financial and operational reporting requirements for home health agencies within the United States. Enforced by federal legislation (42 USC 1395g) and regulatory standards (42 CFR 413.20(b)), this form serves as a comprehensive document that must be submitted to report costs and other financial data pertaining to the services provided by home health agencies. Non-compliance or failure to submit this form can lead to significant financial repercussions, including the requirement to return interim payments deemed as overpayments. The form includes several sections like certification and settlement summaries, identification data, statistical data, and specific sections for rural health clinics or federally qualified health centers when applicable. Its detailed nature requires accurate and truthful reporting under the threat of criminal, civil, and administrative actions for any forms of misrepresentation or falsification. In addition to serving as a tool for financial accountability, the form's structured data collection assists in policy making and regulatory oversight by offering insights into the operational efficiencies and care provision trends among home health agencies. The significant time investment required to complete this form—estimated to average 226 hours—underscores its complexity and the detailed nature of information that agencies must compile and report.
| Question | Answer |
|---|---|
| Form Name | Cms 1728 94 Form |
| Form Length | 57 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 14 min 15 sec |
| Other names | cms 1728 94, cms 1564 cms r 297 printable form, 1728 form printable, dd form 1728 form |
|
|
|
|
FORM |
|
|
3290 (Cont.) |
||||
This report is required by law (42 USC 1395g; 42 CFR 413.20(b)). Failure to report can result |
|
|
|
|
|
||||||
in all interim payments made since the beginning of the cost reporting period being deemed |
|
|
|
FORM APPROVED |
|||||||
as overpayments (42 USC 1395g). |
|
|
|
|
|
|
|
|
OMB NO. |
||
HOME HEALTH AGENCY COST REPORT |
|
|
|
|
PROVIDER CCN: |
PERIOD: |
|
|
|||
CERTIFICATION AND SETTLEMENT SUMMARY |
|
|
|
|
|
From: ___________ |
|
WORKSHEET S |
|||
|
|
|
|
|
|
_______________ |
To: ___________ |
|
|
||
|
Intermediary Use Only: |
|
|
|
|
|
|
|
|
|
|
[ ] |
Audited |
Date Received |
|
____________ |
[ |
] |
Initial |
|
[ ] |
||
[ ] |
Desk Reviewed |
Contractor No. |
____________ |
[ |
] |
Final |
|
|
|||
PART I - CERTIFICATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Check |
|
[ |
] |
Electronically filed cost report |
|
|
Date: ___________ |
|
|
||
applicable box |
[ |
] |
Manually submitted cost report |
|
|
Time: ___________ |
|
|
|||
MISREPRESENTATION OR FALSIFICATION OF ANY INFORMATION CONTAINED IN THIS COST REPORT MAY
BE PUNISHABLE BY CRIMINAL, CIVIL AND ADMINISTRATIVE ACTION, FINE AND/OR IMPRISONMENT
UNDER FEDERAL LAW. FURTHERMORE, IF SERVICES IDENTIFIED IN THIS REPORT WERE PROVIDED
OR PROCURED THROUGH THE PAYMENT DIRECTLY OR INDIRECTLY OF A KICKBACK OR WERE OTHERWISE
ILLEGAL, CRIMINAL, CIVIL AND ADMINISTRATIVE ACTION, FINES AND/OR IMPRISONMENT MAY RESULT.
CERTIFICATION BY OFFICER OR DIRECTOR OF THE AGENCY
IHEREBY CERTIFY that I have read the above certification statement and that I have examined the accompanying electronically filed or manually submitted Home Health Agency Cost Report and the Balance Sheet and Statement of Revenue and Expenses prepared by _________________________________________(Provider name(s) and number(s)) for the cost report beginning _____________________and ending __________________________, and that to the best of my knowledge
and belief, this report and statement are true, correct, complete and prepared from the books and records of the provider in accordance with applicable instructions, except as noted. I further certify that I am familiar with the laws and regulations regarding the provision of health care services, and that the services identified in this cost report were provided in compliance with such laws and regulations.
(Signed) __________________________________________
Officer or Director
__________________________________________
Title
__________________________________________
Date
PART II - SETTLEMENT SUMMARY
|
|
|
TITLE XVIII |
|
|
|
|
PART A |
|
PART B |
|
|
|
1 |
|
2 |
|
1 |
HOME HEALTH AGENCY |
|
|
|
1 |
2 |
HOME |
|
|
|
2 |
3 |
HOME |
|
|
|
3 |
3.5 |
HOME |
|
|
|
3.5 |
|
(specify) |
|
|
|
|
4 |
TOTAL |
|
|
|
4 |
"According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
FORM
Rev. 16 |

3290 (Cont.) |
FORM |
|
|
|
||||||||
HOME HEALTH AGENCY COMPLEX |
|
PROVIDER CCN: |
|
PERIOD: |
|
|
|
|
|
|||
IDENTIFICATION DATA |
|
|
|
From: ___________ |
WORKSHEET |
|
|
|||||
|
|
|
|
________________ |
To: ___________ |
|
|
|
|
|
||
Home Health Agency Complex Address: |
|
|
|
|
|
|
|
|
|
|
||
1 |
Street: |
|
|
P.O. Box: |
|
|
|
|
1 |
|||
1.01 |
City: |
State: |
Zip Code: |
|
|
|
|
1.01 |
||||
Home Health Agency Component Identification |
|
|
|
|
|
|
|
|
|
|
||
|
Contractor No. |
|
|
|
|
|
|
|
|
|
|
|
|
Component |
|
Component Name |
|
Provider No. |
|
Date Certified |
|
|
|||
|
0 |
|
1 |
|
2 |
|
|
3 |
|
|
||
2 |
Home Health Agency |
|
|
|
|
|
|
|
|
|
|
2 |
3 |
|
|
|
|
|
|
|
|
|
|
3 |
|
3.50 |
|
|
|
|
|
|
|
|
|
|
3.50 |
|
4 |
|
|
|
|
|
|
|
|
|
|
4 |
|
5 |
HHA- based RHC |
|
|
|
|
|
|
|
|
|
|
5 |
6 |
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
||||
7 |
Cost Reporting Period (mm/dd/yyyy) |
|
From: ______________ |
To: ______________ |
|
7 |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
Type of control (see instructions) |
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
||||
9 |
If this a low or no Medicare utilization cost report, enter "L" for Low or "N" for No Medicare Utilization. |
|
|
|
|
9 |
||||||
Depreciation: Enter the amount of depreciation reported in this HHA for the methods indicated. |
|
|
|
|
|
|||||||
10 |
Straight Line |
|
|
|
|
|
|
|
|
|
10 |
|
11 |
Declining Balance |
|
|
|
|
|
|
|
|
|
11 |
|
12 |
Sum of the Years' Digits |
|
|
|
|
|
|
|
|
|
12 |
|
13 |
Sum of lines 10, 11 and 12 |
|
|
|
|
|
|
|
|
|
13 |
|
|
|
|
|
|
|
|
|
|
||||
14 |
Were there any disposals of capital assets during this cost reporting period? |
|
|
|
|
14 |
||||||
15 |
Was accelerated depreciation claimed on any assets in the current or any prior cost reporting period? |
|
|
|
|
15 |
||||||
16 |
Was accelerated depreciation claimed on assets acquired on or after August l, l970 (See PRM |
|
|
|
|
16 |
||||||
|
Chapter l)? |
|
|
|
|
|
|
|
|
|
|
|
17 |
If depreciation is funded, enter the balance at end of period. |
|
|
|
|
|
|
|
17 |
|||
18 |
Did the provider cease to participate in the Medicare program at the end of |
|
|
|
|
18 |
||||||
|
the period to which this cost report applies (See PRM |
|
|
|
|
|
||||||
19 |
Was there substantial decrease in health insurance proportion of allowable |
|
|
|
|
19 |
||||||
|
costs from prior cost reporting periods (See PRM |
|
|
|
|
|
|
|
|
|||
20 |
Does the provider qualify as a small HHA (defined in 42 CFR 413.24(d))? |
|
|
|
|
20 |
||||||
21 |
Does the HHA qualify as a nominal charge provider (defined in 42 CFR 409.3)? |
|
|
|
|
21 |
||||||
22 |
Does the HHA contract with outside suppliers for physical therapy services? |
|
|
|
|
22 |
||||||
22.01 |
Does the HHA contract with outside suppliers for occupational therapy services? |
|
|
|
|
22.01 |
||||||
22.02 |
Does the HHA contract with outside suppliers for speech therapy services? |
|
|
|
|
22.02 |
||||||
If this facility contains a |
|
|
|
|
|
|||||||
lower of costs or charges, enter "Y" for each component and type of service that qualifies for the exemption. |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
Part A |
|
Part B |
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
|
|
23 |
HHA |
|
|
|
|
|
|
|
|
|
23 |
|
24 |
CORF |
|
|
|
|
|
|
|
|
|
24 |
|
25 |
CMHC |
|
|
|
|
|
|
|
|
|
25 |
|
26 |
If the HHA componentized (or fragmented) its administrative and general service |
|
|
|
|
26 |
||||||
|
costs, indicate whether option one or option two is being utilized. (See Section 3214) |
|
|
|
|
|
||||||
|
(Enter "1" for option one and "2" for option two) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
27 |
List amounts of malpractice premiums and paid losses: |
|
|
|
|
|
|
|
27 |
|||
27.01 |
Premiums |
|
|
|
|
|
|
|
|
|
27.01 |
|
27.02 |
Paid Losses |
|
|
|
|
|
|
|
|
|
27.02 |
|
27.03 |
Self Insurance |
|
|
|
|
|
|
|
|
|
27.03 |
|
28 |
Are malpractice premiums and/or paid losses reported in other than the Administrative and General |
|
|
|
|
28 |
||||||
|
cost center? If yes, submit a supporting schedule listing cost centers and amounts contained therein. |
|
|
|
|
|
||||||
29 |
If you are part of a chain organization, enter "Y" for yes and enter the name and address of the home |
|
|
|
|
29 |
||||||
FORM |
office, otherwise, enter "N" for no. |
|
|
|
|
|
|
|
|
|
|
|
29.01 |
Home Office Name: |
Home Office No. : |
|
Contractor No. : |
|
|
|
|
29.01 |
|||
29.02 |
Street: |
P.O. Box: |
Contractor Name: |
|
|
|
|
29.02 |
||||
29.03 |
City: |
State: |
Zip Code: |
|
|
|
|
29.03 |
||||
FORM CMS
Rev. 16 |

FORM CM |
3290 (Cont.) |
HOME HEALTH AGENCY STATISTICAL DATA
PROVIDER NO.:
______________
PERIOD:
From: ___________
To: ___________
WORKSHEET
PART I - STATISTICAL DATA |
|
|
COUNTY |
|
Cook |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Title XVIII |
|
Other |
Total |
|
|||
|
DESCRIPTION |
|
Visits |
Patients |
Visits |
|
Patients |
Visits |
Patients |
|
|
|
|
1 |
2 |
3 |
|
4 |
5 |
6 |
|
1 |
Skilled Nursing |
|
|
|
|
|
|
|
|
1 |
2 |
Physical Therapy |
|
|
|
|
|
|
|
|
2 |
3 |
Occupational Therapy |
|
|
|
|
|
|
|
|
3 |
4 |
Speech Pathology |
|
|
|
|
|
|
|
|
4 |
5 |
Medical Social Service |
|
|
|
|
|
|
|
|
5 |
6 |
Home Health Aide |
|
|
|
|
|
|
|
|
6 |
7 |
All Other Services |
|
|
|
|
|
|
|
|
7 |
8 |
Total Visits |
|
|
|
|
|
|
|
|
8 |
9 |
Home Health Aide Hours |
|
|
|
|
|
|
|
|
9 |
10 |
Unduplicated Census Count - |
|
|
|
|
|
|
|
|
10 |
|
Full Cost Reporting Period |
|
|
|
|
|
|
|
|
|
10.01 |
Unduplicated Census Count - |
|
|
|
|
|
|
|
|
10.01 |
|
Pre 10/1/2000 |
|
|
|
|
|
|
|
|
|
10.02 |
Unduplicated Census Count - |
|
|
|
|
|
|
|
|
10.02 |
|
Post 9/30/2000 |
|
|
|
|
|
|
|
|
|
PART II - EMPLOYMENT DATA |
|
|
|
|
|
|
|
|
||
(FULL TIME EQUIVALENT) |
|
|
|
|
|
|
|
|
||
|
Number of hours in |
|
|
|
|
|
|
|
|
|
|
your normal work week __________ |
|
|
|
|
Staff |
Contract |
Total |
|
|
|
|
|
|
|
|
|
1 |
2 |
3 |
|
11 |
Administrator and Assistant Administrator(s) |
|
|
|
|
|
|
11 |
||
12 |
Director and Assistant Director(s) |
|
|
|
|
|
|
|
12 |
|
13 |
Other Administrative Personnel |
|
|
|
|
|
|
|
13 |
|
14 |
Direct Nursing Service |
|
|
|
|
|
|
|
14 |
|
15 |
Nursing Supervisor |
|
|
|
|
|
|
|
15 |
|
16 |
Physical Therapy Service |
|
|
|
|
|
|
|
16 |
|
17 |
Physical Therapy Supervisor |
|
|
|
|
|
|
|
17 |
|
18 |
Occupational Therapy Service |
|
|
|
|
|
|
|
18 |
|
19 |
Occupational Therapy Supervisor |
|
|
|
|
|
|
|
19 |
|
20 |
Speech Pathology Service |
|
|
|
|
|
|
|
20 |
|
21 |
Speech Pathology Supervisor |
|
|
|
|
|
|
|
21 |
|
22 |
Medical Social Service |
|
|
|
|
|
|
|
22 |
|
23 |
Medical Social Supervisor |
|
|
|
|
|
|
|
23 |
|
24 |
Home Health Aide |
|
|
|
|
|
|
|
24 |
|
25 |
Home Health Aide Supervisor |
|
|
|
|
|
|
|
25 |
|
26 |
|
|
|
|
|
|
|
|
|
26 |
27 |
|
|
|
|
|
|
|
|
|
27 |
PART III - METROPOLITAN STATISTICAL AREA (MSA) AND CORE BASED STATISTICAL AREA (CBSA) CODES |
||||||||||
|
|
|
|
|
|
|
|
1 |
1.01 |
|
|
Enter the total number of MSAs in column 1 and/or CBSAs in column 2 where Medicare |
|
|
|
||||||
28 |
covered services were provided during the cost reporting period. |
|
|
|
|
|
28 |
|||
|
List all MSA and CBSA codes in which Medicare covered home health services were |
MSA Codes |
CBSA Codes |
|
||||||
29 |
provided during the cost reporting period (line 29 contains the first code): |
|
|
|
|
29 |
||||
|
|
|
|
|
|
|
|
|
|
29.01 |
|
|
|
|
|
|
|
|
|
|
29.02 |
|
|
|
|
|
|
|
|
|
|
29.03 |
|
|
|
|
|
|
|
|
|
|
29.04 |
|
|
|
|
|
|
|
|
|
|
29.05 |
|
|
|
|
|
|
|
|
|
|
29.06 |
|
|
|
|
|
|
|
|
|
|
29.07 |
|
|
|
|
|
|
|
|
|
|
29.08 |
|
|
|
|
|
|
|
|
|
|
29.09 |
FORM
Rev. 13 |
3290 (Cont.) |
FORM CM |
HOME HEALTH AGENCY STATISTICAL DATA
PROVIDER NO.:
______________
PERIOD:
From: ______________
To: ______________
WORKSHEET
PART IV - PPS ACTIVITY DATA - Applicable for Services Rendered on or After October 1, 2000 |
|
|
Cook |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Full Episodes |
Full Episodes |
LUPA Episodes |
PEP Only |
SCIC within a |
SCIC Only |
Totals |
|
|
DESCRIPTION |
without Outliers |
with Outliers |
|
Episodes |
PEP |
Episodes |
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
30 |
Skilled Nursing Visits |
|
|
|
|
|
|
|
30 |
31 |
Skilled Nursing Visit Charges |
|
|
|
|
|
|
|
31 |
32 |
Physical Therapy Visits |
|
|
|
|
|
|
|
32 |
33 |
Physical Therapy Visit Charges |
|
|
|
|
|
|
|
33 |
34 |
Occupational Therapy Visits |
|
|
|
|
|
|
|
34 |
35 |
Occupational Therapy Visit Charges |
|
|
|
|
|
|
|
35 |
36 |
Speech Pathology Visits |
|
|
|
|
|
|
|
36 |
37 |
Speech Pathology Visit Charges |
|
|
|
|
|
|
|
37 |
38 |
Medical Social Service Visits |
|
|
|
|
|
|
|
38 |
39 |
Medical Social Service Visit Charges |
|
|
|
|
|
|
|
39 |
40 |
Home Health Aide Visits |
|
|
|
|
|
|
|
40 |
41 |
Home Health Aide Visit Charges |
|
|
|
|
|
|
|
41 |
42 |
Total Visits (Sum of lines 30,32,34,36,38,40) |
|
|
|
|
|
|
|
42 |
43 |
Other Charges |
|
|
|
|
|
|
|
43 |
44 |
Total Charges (Sum of lines 31,33,35,37,39,41,43) |
|
|
|
|
|
|
|
44 |
45 |
Total Number of Episodes |
|
|
|
|
|
|
|
45 |
46 |
Total Number of Outlier Episodes |
|
|
|
|
|
|
|
46 |
47 |
Total |
|
|
|
|
|
|
|
47 |
FORM
Rev. 13 |

|
|
FORM CM |
|
|
|
3290 (Cont.) |
|||
|
PROVIDER CCN: |
PERIOD: |
|
WORKSHEET |
|||||
FEDERALLY QUALIFIED HEALTH CENTER |
|
_____________ |
FROM: __________ |
|
|
||||
PROVIDER STATISTICAL DATA |
|
COMPONENT CCN: |
TO: ___________ |
|
|
||||
|
|
|
|
_____________ |
|
|
|
|
|
Check |
|
[ ] RHC |
|
|
|
|
|
|
|
Applicable Box |
[ ] FQHC |
|
|
|
|
|
|
|
|
Clinic Address and Identification: |
|
|
|
|
|
|
|
||
1 |
Street: |
|
|
|
|
|
|
|
1 |
1.01 |
City: |
|
|
State: |
Zip Code: |
County: |
|
1.01 |
|
2 |
Designation (for FQHCs only) - Enter "R" for rural or "U" for urban |
|
|
|
|
2 |
|||
|
|
|
|
|
|
|
|
|
|
Source of Federal Funds: |
|
|
|
|
|
Grant Award |
Date |
|
|
|
|
|
|
|
|
|
1 |
2 |
|
3 |
Community Health Center (Section 330(d), PHS Act) |
|
|
|
|
|
|
3 |
|
4 |
Migrant Health Center (Section 329(d), PHS Act) |
|
|
|
|
|
|
4 |
|
5 |
Health Services for the Homeless (Section 340(d), PHS Act) |
|
|
|
|
5 |
|||
6 |
Appalachian Regional Commission |
|
|
|
|
|
|
6 |
|
7 |
|
|
|
|
|
|
|
7 |
|
8 |
Other (specify) |
|
|
|
|
|
|
|
8 |
Physician Information: |
Physician |
Billing |
|
|
|
Name |
Number |
9 |
Physician(s) furnishing services at the clinic or under agreement (see instructions) |
|
|
9
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician |
Hours of |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
Supervision |
|
||
10 |
Supervisory physician(s) and hours of supervision during period (see instructions) |
|
|
|
|
|
|
|
10 |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
11 |
Does the facility operate as other than an RHC or FQHC? If yes, indicate number of other operations in column 2 and |
|
|
11 |
|||||||||||||
|
list the other type(s) of operation(s) and hours on subscripts of line 12. |
|
|
|
|
|
|
|
|
|
|
||||||
|
Enter the clinic hours on line 12 and list the other type(s) of operation(s) and hours on subscripts of line 12. (1) |
|
|
|
|
||||||||||||
|
|
Sunday |
Monday |
Tuesday |
Wednesday |
Thursday |
Friday |
Saturday |
|
||||||||
|
|
from |
to |
from |
to |
from |
to |
from |
|
to |
from |
to |
from |
to |
from |
to |
|
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
8 |
9 |
10 |
11 |
12 |
13 |
14 |
|
12 |
Clinic |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 |
12.01 |
Specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12.01 |
12.02 |
Specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12.02 |
12.03 |
Specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12.03 |
(1) List hours of operation based on a 24 hour clock. For example, 8:30am is 0830, 5:30pm is 1730 and 12 midnight is 2400.
13 |
Has the facility been approved for an exception to the productivity standard? |
|
|
|
13 |
|
14 |
Is this a consolidated cost report as defined in CMS Pub. 27, section 508(D)? If yes, enter in column 2 the |
|
|
|
14 |
|
|
number of providers included in this report. List all provider names and numbers below. |
|
|
|
|
|
15 |
Provider name: ______________________________ |
Provider number: _______________ |
|
|
|
15 |
15.01 |
Provider name: ______________________________ |
Provider number: _______________ |
|
|
|
15.01 |
15.02 |
Provider name: ______________________________ |
Provider number: _______________ |
|
|
|
15.02 |
15.03 |
Provider name: ______________________________ |
Provider number: _______________ |
|
|
|
15.03 |
16 |
Are you claiming allowable GME costs as a result of "substantial payment" for interns |
Y/N |
XVIII |
TOTAL |
16 |
|
|
and residents? If yes, enter the number of Medicare visits in column 2 and total visits in column 3 |
1 |
2 |
3 |
|
|
|
performed by interns and residents and complete Worksheet |
|
|
|
|
|
FORM
Rev. 16 |

3290 (CONT.) |
FORM |
HOSPICE IDENTIFICATION DATA
PROVIDER CCN:
_____________
HOSPICE CCN:
_____________
PERIOD:
FROM: _____________
TO: ________________
WORKSHEET
PART I
|
|
|
Title XVIII |
|
Total |
|
|
|
|
|
|
Unduplicated |
|
Unduplicated |
|
|
|
|
|
Skilled |
Other |
Days |
|
|
|
|
Unduplicated |
Nursing |
Unduplicated |
(sum of |
|
|
|
Enrollment Days |
Days |
Facility Days |
Days |
cols. 1 & 3) |
|
|
|
|
1 |
2 |
3 |
4 |
|
1 |
Continuous Home Care |
|
|
|
|
1 |
|
2 |
Routine Home Care |
|
|
|
|
2 |
|
3 |
Inpatient Respite Care |
|
|
|
|
3 |
|
4 |
General Inpatient Care |
|
|
|
|
4 |
|
5 |
Total Hospice Days |
|
|
|
|
5 |
|
PART I I |
|
|
|
|
|
||
|
|
|
|
Title XVIII |
|
|
|
|
|
|
|
Skilled |
|
Total |
|
|
|
|
|
Nursing |
|
(sum of |
|
|
|
Census Data |
Title XVIII |
Facility |
Other |
cols. 1 & 3) |
|
|
|
|
1 |
2 |
3 |
4 |
|
6 |
Number of Patients Receiving |
|
|
|
|
6 |
|
|
Hospice Care |
|
|
|
|
|
|
7 |
Total Number of Unduplicated |
|
|
|
|
7 |
|
|
Continuous Care Hours |
|
|
|
|
|
|
|
Billable to Medicare |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
Average |
Length of Stay (line 5 divided by line 6) |
|
|
|
|
8 |
9 |
Unduplicated Census Count |
|
|
|
|
9 |
|
NOTE: Parts I & II, column 1 also includes the days reported in column 2.
FORM
SECTIONS 3239 - 3239.2)
REV. 16 |

|
|
FORM CM |
|
|
|
|
|
|
3290 (Cont.) |
||||||
|
PROVIDER NO.: _______________ |
|
|
PERIOD: |
|
|
|
|
SUPPLEMENTAL |
||||||
|
|
|
CORF NO.: _______________ |
|
|
From: ___________ |
|
|
|
WORKSHEET |
|||||
|
|
|
|
|
|
To: ___________ |
|
|
|
|
|
|
|
||
|
CORF TREATMENTS |
|
|
|
Title XVIII |
|
Other |
|
Total |
|
|
||||
|
|
|
|
|
Treatments |
|
Patients |
Treatments |
|
Patients |
Treatments |
|
Patients |
|
|
|
|
|
|
|
1 |
|
2 |
3 |
|
4 |
5 |
|
6 |
|
|
1 |
Skilled Nursing Care |
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
Physical Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
3 |
Occupational Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
4 |
Speech Pathology |
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
5 |
Medical Social Services |
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
6 |
Respiratory Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
7 |
Psychological Services |
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
8 |
All Other Service |
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
9 |
Total Treatments (Sum of lines |
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
CORF - NUMBER OF EMPLOYEES ( FULL TIME EQUIVALENT ) |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Enter the number of hours |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
in your normal workweek |
__________ |
|
|
Staff |
|
Contract |
|
Total |
|
|
||||
|
|
|
|
|
1 |
|
|
2 |
|
3 |
|
|
|
||
10 |
Administrators and Assistant Administrators |
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
11 |
Directors and Assistant Directors |
|
|
|
|
|
|
|
|
|
|
|
|
11 |
|
12 |
Other Administrative Personnel |
|
|
|
|
|
|
|
|
|
|
|
|
12 |
|
13 |
Direct Nursing Service |
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|
14 |
Nursing Supervisor |
|
|
|
|
|
|
|
|
|
|
|
|
14 |
|
15 |
Physical Therapy Service |
|
|
|
|
|
|
|
|
|
|
|
|
15 |
|
16 |
Physical Therapy Supervisor |
|
|
|
|
|
|
|
|
|
|
|
|
16 |
|
17 |
Occupational Therapy Service |
|
|
|
|
|
|
|
|
|
|
|
|
17 |
|
18 |
Occupational Therapy Supervisor |
|
|
|
|
|
|
|
|
|
|
|
|
18 |
|
19 |
Speech Pathology Service |
|
|
|
|
|
|
|
|
|
|
|
|
19 |
|
20 |
Speech Pathology Supervisor |
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
21 |
Medical Social Service |
|
|
|
|
|
|
|
|
|
|
|
|
21 |
|
22 |
Medical Social Supervisor |
|
|
|
|
|
|
|
|
|
|
|
|
22 |
|
23 |
Respiratory Therapy Service |
|
|
|
|
|
|
|
|
|
|
|
|
23 |
|
24 |
Respiratory Therapy Supervisor |
|
|
|
|
|
|
|
|
|
|
|
|
24 |
|
25 |
Psychological Service |
|
|
|
|
|
|
|
|
|
|
|
|
25 |
|
26 |
Psychological Service Supervisor |
|
|
|
|
|
|
|
|
|
|
|
|
26 |
|
27 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27 |
28 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28 |
FORM CMS
Rev. 13 |
3290 (Cont.) |
|
|
|
FORM |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
PROVIDER NO.: |
PERIOD: |
|
|
|
||
|
|
RECLASSIFICATION AND ADJUSTMENT OF TRIAL BALANCE OF EXPENSES |
|
|
_______________ |
From: ___________ |
WORKSHEET A |
|||||||
|
|
|
|
|
|
|
|
|
|
To: ___________ |
|
|
|
|
|
|
|
|
|
|
CONTRACTED |
|
|
|
RECLASSI- |
|
|
EXPENSES |
|
|
|
|
|
EMPLOYEE |
TRANSPOR- |
PURCHASED |
|
|
RECLASSI- |
FIED TRIAL |
|
|
FOR COST |
|
|
|
|
SALARIES |
BENEFITS |
TATION (See |
SERVICES |
OTHER |
|
FICATION |
BALANCE |
|
ADJUST- |
ALLOCATION |
|
|
|
|
(Fr Wks |
(Fr Wks |
Instructions) |
(Fr Wks |
COSTS |
TOTAL |
(Fr Wks |
(Cols 6 + 7) |
|
MENTS |
(Col 8 + 9) |
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
|
|
|
GENERAL SERVICE COST CENTER |
|
|
|
|
|
|
|
|
|
|
|
|
1 |
0100 |
Capital Related - Bldg. & Fix. |
|
|
|
|
|
|
|
|
|
|
|
1 |
2 |
0200 |
Capital Related - Movable Equip |
|
|
|
|
|
|
|
|
|
|
|
2 |
3 |
0300 |
Plant Operation & Maintenance |
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
0400 |
Transportation (See Instructions) |
|
|
|
|
|
|
|
|
|
|
|
4 |
5 |
0500 |
Administrative and General |
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
HHA REIMBURSABLE SERVICES |
|
|
|
|
|
|
|
|
|
|
|
|
6 |
0600 |
Skilled Nursing Care |
|
|
|
|
|
|
|
|
|
|
|
6 |
7 |
0700 |
Physical Therapy |
|
|
|
|
|
|
|
|
|
|
|
7 |
8 |
0800 |
Occupational Therapy |
|
|
|
|
|
|
|
|
|
|
|
8 |
9 |
0900 |
Speech Pathology |
|
|
|
|
|
|
|
|
|
|
|
9 |
10 |
1000 |
Medical Social Services |
|
|
|
|
|
|
|
|
|
|
|
10 |
11 |
1100 |
Home Health Aide |
|
|
|
|
|
|
|
|
|
|
|
11 |
12 |
1200 |
Supplies (See Instructions) |
|
|
|
|
|
|
|
|
|
|
|
12 |
13 |
1300 |
Drugs |
|
|
|
|
|
|
|
|
|
|
|
13 |
13.20 |
1320 |
Cost of Administering Vaccines |
|
|
|
|
|
|
|
|
|
|
|
13.20 |
14 |
1400 |
DME |
|
|
|
|
|
|
|
|
|
|
|
14 |
|
|
HHA NONREIMBURSABLE SERVICES |
|
|
|
|
|
|
|
|
|
|
|
|
15 |
1500 |
Home Dialysis Aide Services |
|
|
|
|
|
|
|
|
|
|
|
15 |
16 |
1600 |
Respiratory Therapy |
|
|
|
|
|
|
|
|
|
|
|
16 |
17 |
1700 |
Private Duty Nursing |
|
|
|
|
|
|
|
|
|
|
|
17 |
18 |
1800 |
Clinic |
|
|
|
|
|
|
|
|
|
|
|
18 |
19 |
1900 |
Health Promotion Activities |
|
|
|
|
|
|
|
|
|
|
|
19 |
20 |
2000 |
Day Care Program |
|
|
|
|
|
|
|
|
|
|
|
20 |
21 |
2100 |
Home Delivered Meals Program |
|
|
|
|
|
|
|
|
|
|
|
21 |
22 |
2200 |
Homemaker |
|
|
|
|
|
|
|
|
|
|
|
22 |
23 |
|
Other |
|
|
|
|
|
|
|
|
|
|
|
23 |
|
|
SPECIAL PURPOSE COST CENTERS |
|
|
|
|
|
|
|
|
|
|
|
|
24 |
2400 |
CORF |
|
|
|
|
|
|
|
|
|
|
|
24 |
25 |
2500 |
Hospice |
|
|
|
|
|
|
|
|
|
|
|
25 |
26 |
2600 |
CMHC |
|
|
|
|
|
|
|
|
|
|
|
26 |
27 |
2700 |
RHC |
|
|
|
|
|
|
|
|
|
|
|
27 |
28 |
2800 |
FQHC |
|
|
|
|
|
|
|
|
|
|
|
28 |
29 |
|
Total |
|
|
|
|
|
|
|
|
|
|
|
29 |
FORM
Rev. 13 |

|
|
|
FORM CM |
|
|
|
|
3290 (Cont.) |
||||||
COMPENSATION ANALYSIS |
|
|
|
|
PROVIDER NO.: |
|
PERIOD: |
|
|
|
||||
SALARIES AND WAGES |
|
|
|
|
_______________ |
From: ___________ |
|
WORKSHEET |
||||||
|
|
|
|
|
|
|
|
|
|
To: ___________ |
|
|
|
|
|
|
ADMINIS- |
|
|
|
|
|
|
|
|
|
ALL |
TOTAL |
|
|
|
TRATORS |
DIRECTORS |
CONSULTANTS |
SUPERVISORS |
NURSES |
|
THERAPISTS |
AIDES |
|
OTHER |
(1) |
|
|
|
|
1 |
2 |
3 |
|
4 |
5 |
|
6 |
7 |
|
8 |
9 |
|
|
GENERAL SERVICE COST CENTER |
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
Capital Related - Bldg. and Fixtures |
|
|
|
|
|
|
|
|
|
|
|
|
1 |
2 |
Capital Related - Movable Equipment |
|
|
|
|
|
|
|
|
|
|
|
|
2 |
3 |
Plant Operation & Maintenance |
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
Transportation (See Instructions) |
|
|
|
|
|
|
|
|
|
|
|
|
4 |
5 |
Administrative and General |
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
HHA REIMBURSABLE SERVICES |
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
Skilled Nursing Care |
|
|
|
|
|
|
|
|
|
|
|
|
6 |
7 |
Physical Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
7 |
8 |
Occupational Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
8 |
9 |
Speech Pathology |
|
|
|
|
|
|
|
|
|
|
|
|
9 |
10 |
Medical Social Services |
|
|
|
|
|
|
|
|
|
|
|
|
10 |
11 |
Home Health Aide |
|
|
|
|
|
|
|
|
|
|
|
|
11 |
12 |
Supplies |
|
|
|
|
|
|
|
|
|
|
|
|
12 |
13 |
Drugs |
|
|
|
|
|
|
|
|
|
|
|
|
13 |
14 |
DME |
|
|
|
|
|
|
|
|
|
|
|
|
14 |
|
HHA NONREIMBURSABLE SERVICES |
|
|
|
|
|
|
|
|
|
|
|
|
|
15 |
Home Dialysis Aide Services |
|
|
|
|
|
|
|
|
|
|
|
|
15 |
16 |
Respiratory Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
16 |
17 |
Private Duty Nursing |
|
|
|
|
|
|
|
|
|
|
|
|
17 |
18 |
Clinic |
|
|
|
|
|
|
|
|
|
|
|
|
18 |
19 |
Health Promotion Activities |
|
|
|
|
|
|
|
|
|
|
|
|
19 |
20 |
Day Care Program |
|
|
|
|
|
|
|
|
|
|
|
|
20 |
21 |
Home Delivered Meals Program |
|
|
|
|
|
|
|
|
|
|
|
|
21 |
22 |
Homemaker Service |
|
|
|
|
|
|
|
|
|
|
|
|
22 |
23 |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
23 |
|
SPECIAL PURPOSE COST CENTERS |
|
|
|
|
|
|
|
|
|
|
|
|
|
24 |
CORF |
|
|
|
|
|
|
|
|
|
|
|
|
24 |
25 |
Hospice |
|
|
|
|
|
|
|
|
|
|
|
|
25 |
26 |
CMHC |
|
|
|
|
|
|
|
|
|
|
|
|
26 |
27 |
RHC |
|
|
|
|
|
|
|
|
|
|
|
|
27 |
28 |
FQHC |
|
|
|
|
|
|
|
|
|
|
|
|
28 |
29 |
Total |
|
|
|
|
|
|
|
|
|
|
|
|
29 |
(1) Transfer the amounts in column 9 to Wkst. A, column 1
FORM
Rev. 7 |

3290 (Cont.) |
|
FORM CM |
|
|
|
|
|||||||
COMPENSATION ANALYSIS |
|
|
|
PROVIDER NO.: |
|
PERIOD: |
|
|
|
||||
EMPLOYEE BENEFITS (PAYROLL RELATED) |
|
|
|
_______________ |
From: ___________ |
|
WORKSHEET |
||||||
|
|
|
|
|
|
|
|
|
To: ___________ |
|
|
|
|
|
|
ADMINIS- |
|
|
|
|
|
|
|
|
ALL |
TOTAL |
|
|
|
TRATORS |
DIRECTORS |
CONSULTANTS |
SUPERVISORS |
NURSES |
|
THERAPISTS |
AIDES |
|
OTHER |
(1) |
|
|
|
1 |
2 |
3 |
4 |
5 |
|
6 |
7 |
|
8 |
9 |
|
|
GENERAL SERVICE COST CENTER |
|
|
|
|
|
|
|
|
|
|
|
|
1 |
Capital Related - Bldg. and Fixtures |
|
|
|
|
|
|
|
|
|
|
|
1 |
2 |
Capital Related - Movable Equipment |
|
|
|
|
|
|
|
|
|
|
|
2 |
3 |
Plant Operation & Maintenance |
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
Transportation (See Instructions) |
|
|
|
|
|
|
|
|
|
|
|
4 |
5 |
Administrative and General |
|
|
|
|
|
|
|
|
|
|
|
5 |
|
HHA REIMBURSABLE SERVICES |
|
|
|
|
|
|
|
|
|
|
|
|
6 |
Skilled Nursing Care |
|
|
|
|
|
|
|
|
|
|
|
6 |
7 |
Physical Therapy |
|
|
|
|
|
|
|
|
|
|
|
7 |
8 |
Occupational Therapy |
|
|
|
|
|
|
|
|
|
|
|
8 |
9 |
Speech Pathology |
|
|
|
|
|
|
|
|
|
|
|
9 |
10 |
Medical Social Services |
|
|
|
|
|
|
|
|
|
|
|
10 |
11 |
Home Health Aide |
|
|
|
|
|
|
|
|
|
|
|
11 |
12 |
Supplies |
|
|
|
|
|
|
|
|
|
|
|
12 |
13 |
Drugs |
|
|
|
|
|
|
|
|
|
|
|
13 |
14 |
DME |
|
|
|
|
|
|
|
|
|
|
|
14 |
|
HHA NONREIMBURSABLE SRVS |
|
|
|
|
|
|
|
|
|
|
|
|
15 |
Home Dialysis Aide Services |
|
|
|
|
|
|
|
|
|
|
|
15 |
16 |
Respiratory Therapy |
|
|
|
|
|
|
|
|
|
|
|
16 |
17 |
Private Duty Nursing |
|
|
|
|
|
|
|
|
|
|
|
17 |
18 |
Clinic |
|
|
|
|
|
|
|
|
|
|
|
18 |
19 |
Health Promotion Activities |
|
|
|
|
|
|
|
|
|
|
|
19 |
20 |
Day Care Program |
|
|
|
|
|
|
|
|
|
|
|
20 |
21 |
Home Delivered Meals Program |
|
|
|
|
|
|
|
|
|
|
|
21 |
22 |
Homemaker Services |
|
|
|
|
|
|
|
|
|
|
|
22 |
23 |
Other |
|
|
|
|
|
|
|
|
|
|
|
23 |
|
SPECIAL PURPOSE COST CENTERS |
|
|
|
|
|
|
|
|
|
|
|
|
24 |
CORF |
|
|
|
|
|
|
|
|
|
|
|
24 |
25 |
Hospice |
|
|
|
|
|
|
|
|
|
|
|
25 |
26 |
CMHC |
|
|
|
|
|
|
|
|
|
|
|
26 |
27 |
RHC |
|
|
|
|
|
|
|
|
|
|
|
27 |
28 |
FQHC |
|
|
|
|
|
|
|
|
|
|
|
28 |
29 |
Total |
|
|
|
|
|
|
|
|
|
|
|
29 |
(1) Transfer the amounts in column 9 to Wkst. A, column 2
FORM
Rev. 7 |