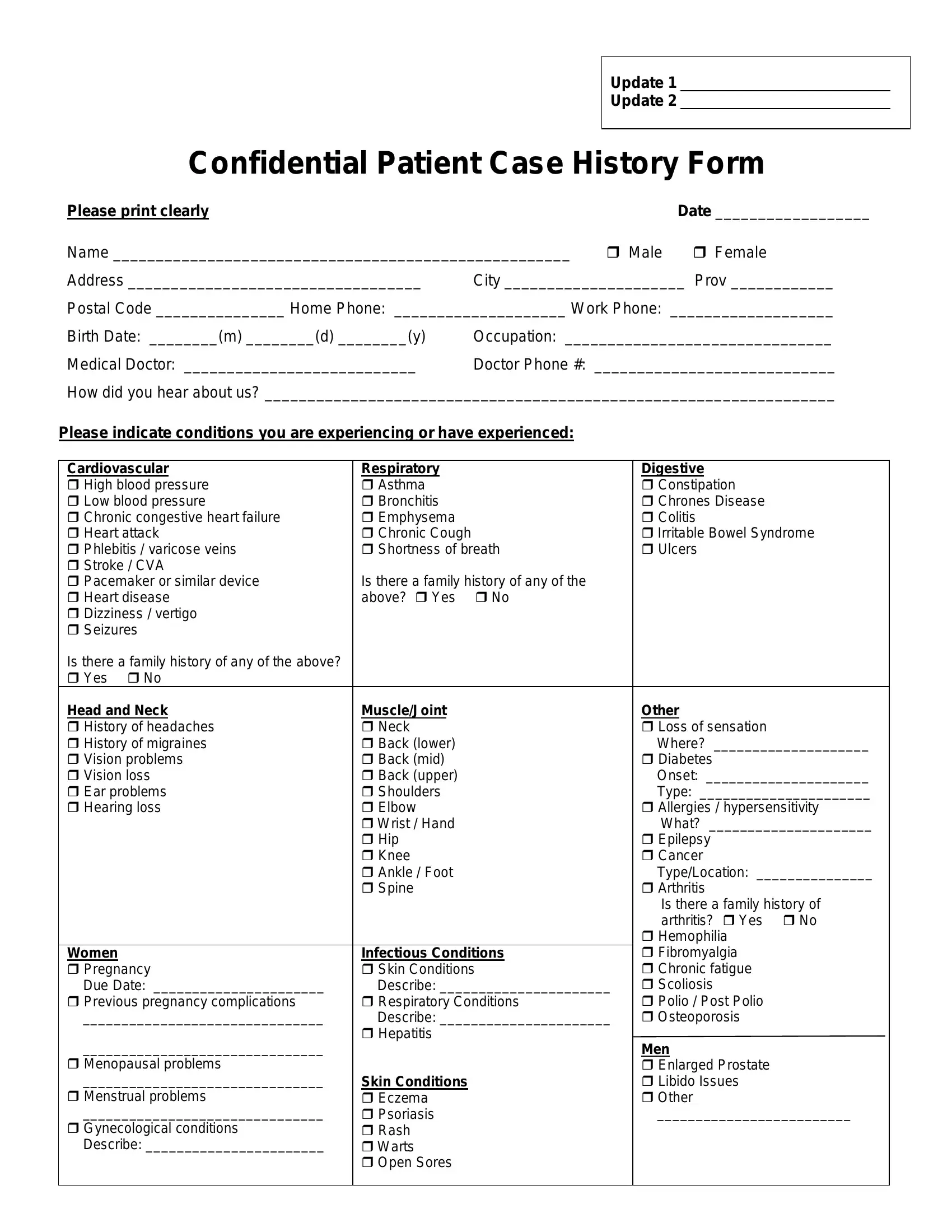
When stepping into a healthcare provider's office, particularly for massage therapy, one typically encounters various forms of paperwork that need to be filled out before treatment can begin. Among these, the Confidential Patient Case History Form plays a crucial role in ensuring that the care provided is tailored to the specific needs and health conditions of the patient. Designed to gather comprehensive personal and medical information, this form asks for basic identifiers like name, address, and contact information, while also diving deep into medical history details. Patients are prompted to disclose conditions ranging from cardiovascular and respiratory issues to digestive ailments and beyond. It meticulously inquires about family medical history, surgeries undergone, medication intake, and even lifestyle factors such as levels of physical, mental, and emotional satisfaction. This meticulous compilation of data not only aids therapists in customizing treatment plans but also flags any potential risks or precautions to be considered during therapy. Significantly, it underscores the importance of mutual understanding and agreement between the therapist and patient regarding the scope of treatment, clearly stating the non-diagnostic role of massage therapists. By providing a thorough snapshot of the patient's health, this form acts as a cornerstone for effective and safe therapeutic practices.
| Question | Answer |
|---|---|
| Form Name | Confidential Patient Case History Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Prov, CVA, case history format pdf, RMT |
Update 1
Update 2
Confidential Patient Case History Form
Please print clearly |
|
|
Date __________________ |
Name _____________________________________________________ |
Male |
Female |
|
Address __________________________________ |
City _____________________ Prov ____________ |
||
Postal Code _______________ Home Phone: ____________________ Work Phone: ___________________
Birth Date: ________(m) ________(d) ________(y) |
Occupation: _______________________________ |
Medical Doctor: ___________________________ |
Doctor Phone #: ____________________________ |
How did you hear about us? __________________________________________________________________
Please indicate conditions you are experiencing or have experienced:
Cardiovascular |
Respiratory |
Digestive |
High blood pressure |
Asthma |
Constipation |
Low blood pressure |
Bronchitis |
Chrones Disease |
Chronic congestive heart failure |
Emphysema |
Colitis |
Heart attack |
Chronic Cough |
Irritable Bowel Syndrome |
Phlebitis / varicose veins |
Shortness of breath |
Ulcers |
Stroke / CVA |
|
|
Pacemaker or similar device |
Is there a family history of any of the |
|
Heart disease |
above? Yes No |
|
Dizziness / vertigo |
|
|
Seizures |
|
|
Is there a family history of any of the above? |
|
|
Yes No |
|
|
Head and Neck |
Muscle/Joint |
Other |
History of headaches |
Neck |
Loss of sensation |
History of migraines |
Back (lower) |
Where? ____________________ |
Vision problems |
Back (mid) |
Diabetes |
Vision loss |
Back (upper) |
Onset: _____________________ |
Ear problems |
Shoulders |
Type: ______________________ |
Hearing loss |
Elbow |
Allergies / hypersensitivity |
|
Wrist / Hand |
What? _____________________ |
|
Hip |
Epilepsy |
|
Knee |
Cancer |
|
Ankle / Foot |
Type/Location: _______________ |
|
Spine |
Arthritis |
|
|
Is there a family history of |
|
|
arthritis? Yes No |
|
|
Hemophilia |
Women |
Infectious Conditions |
Fibromyalgia |
Pregnancy |
Skin Conditions |
Chronic fatigue |
Due Date: ______________________ |
Describe: ______________________ |
Scoliosis |
Previous pregnancy complications |
Respiratory Conditions |
Polio / Post Polio |
_______________________________ |
Describe: ______________________ |
Osteoporosis |
_______________________________ |
Hepatitis |
Men |
|
||
Menopausal problems |
|
Enlarged Prostate |
_______________________________ |
Skin Conditions |
Libido Issues |
Menstrual problems |
Eczema |
Other |
_______________________________ |
Psoriasis |
_________________________ |
Gynecological conditions |
Rash |
|
Describe: _______________________ |
Warts |
|
|
Open Sores |
|
|
|
|
Do you have any medical conditions not listed above? Yes No
If yes, please describe: ________________________________________________________________________
Do you have any internal wires, artificial joints, pacemakers or special equipment that we should be aware of? Yes No
___________________________________________________________________________________________
Please circle areas which are currently causing you symptoms of pain, stiffness, numbness or other forms of discomfort
Face |
Upper back |
Arm(s) |
Hand(s) |
Thigh(s) |
Ankle(s) |
Neck |
Mid back |
Elbow(s) |
Finger(s) |
Knee(s) |
Feet |
Shoulder(s) |
Lower back |
Wrist(s) |
Hip(s) |
Leg(s) |
Toe(s) |
Chest |
Ribs |
Tailbone |
For what condition or reason are you seeking treatment today? ____________________________________
___________________________________________________________________________________________
Have you seen any other health care professional(s) for this condition or reason? Yes No If yes whom? ________________________________________________________
Have you ever been involved in any motor vehicle accidents? Yes |
No Date:___________________ |
|
Have you been involved in any other accidents? |
Yes |
No Date:___________________ |
Have you ever been knocked unconscious? |
Yes |
No Date:___________________ |
Briefly list any surgeries you have undergone, for what and when.
___________________________________________________________________________________________
___________________________________________________________________________________________
Are you presently taking any prescribed medication(s)? Yes No
If yes, please list the medication(s) and the condition(s) for which it is being used if known.
___________________________________________________________________________________________
___________________________________________________________________________________________
Have you previously received massage therapy treatments? |
Yes No |
If yes, were you treated: |
At this clinic From an RMT Other |
Please circle on the following scales the extent to which you are currently satisfied with the following:
(5 represents total satisfaction, 1 represents little or no satisfaction)
Physical health & fitness |
5 |
4 |
3 |
2 |
1 |
Mental & emotional happiness |
5 |
4 |
3 |
2 |
1 |
Energy level |
5 |
4 |
3 |
2 |
1 |
Diet |
5 |
4 |
3 |
2 |
1 |
Ability to relax |
5 |
4 |
3 |
2 |
1 |
I acknowledge that the Massage Therapist is not a physician and does not diagnose illness or disease or any other physical or mental disorder. I clearly understand that massage therapy is not a substitute for a medical examination. It is recommended that I attend my personal physician for any ailment that I may be experiencing. I acknowledge that no assurance or guarantee has been provided to me as to the results of the treatment.
I acknowledge and understand that the Massage Therapist must be fully aware of my existing medical conditions. I have completed my medical history form as provided by my Massage Therapist and disclosed all of those medical conditions affecting me. It is my responsibility to keep the Massage Therapist updated on my medical history. The information I have provided is true and complete to the best of my knowledge.
_____________________________________________ |
____________________ |
________________________ |
Signature |
Date |
Therapist Signature |
_____________________________________________ |
____________________ |
________________________ |
Signature |
Date |
Therapist Signature |
_____________________________________________ |
____________________ |
________________________ |
Signature |
Date |
Therapist Signature |