



Our PDF editor was made to be as easy as possible. As soon as you adhere to the following steps, the procedure for filling out the blank contact lens prescription form file will be simple and easy.
Step 1: You can click the orange "Get Form Now" button at the top of this web page.
Step 2: Right now, you may modify the blank contact lens prescription form. The multifunctional toolbar will let you add, get rid of, customize, highlight, as well as carry out similar commands to the content and fields inside the document.
The PDF file you plan to complete will consist of the following segments:
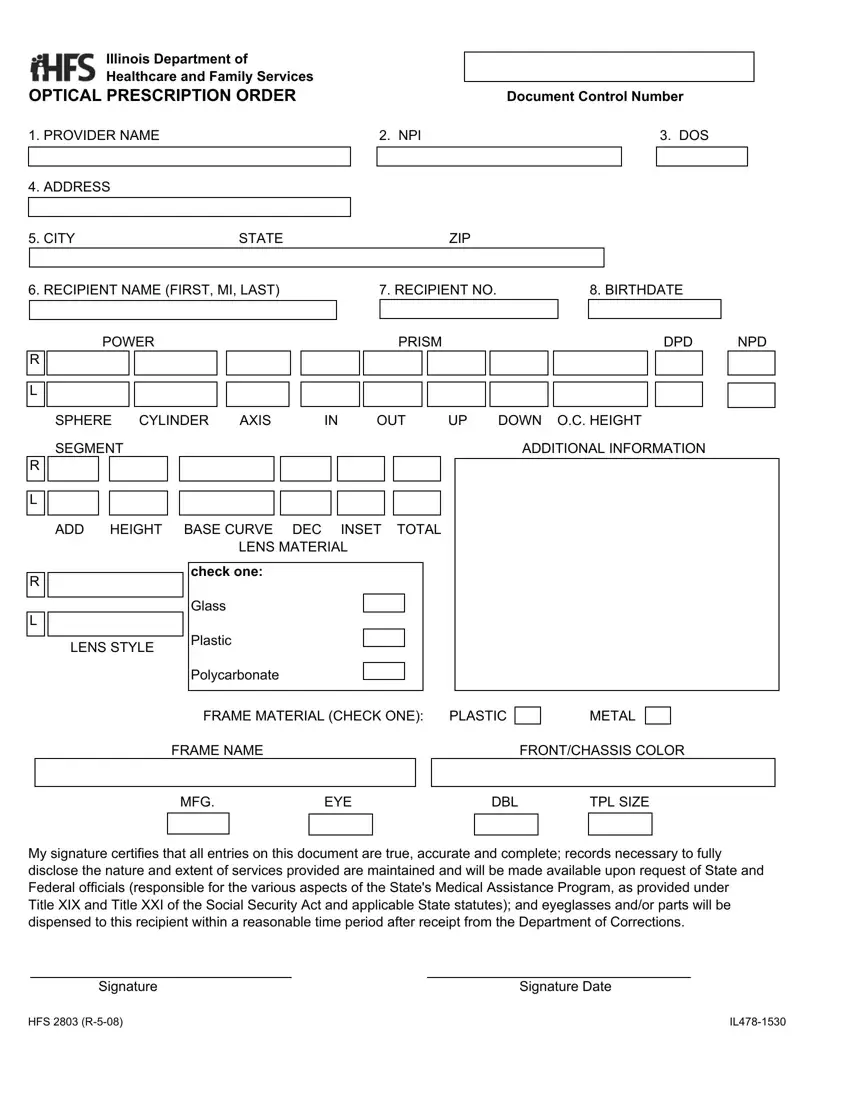
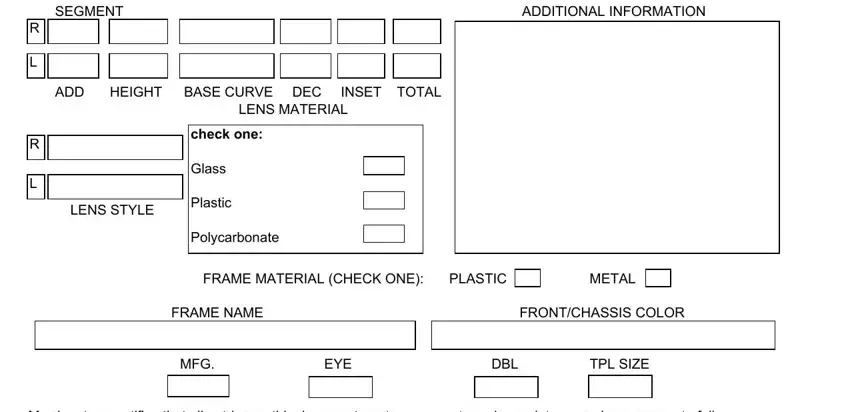
Provide the required details in the SEGMENT, ADDITIONAL INFORMATION, ADD, HEIGHT, BASE CURVE DEC, INSET, TOTAL, LENS MATERIAL, check one, Glass, Plastic, Polycarbonate, LENS STYLE, FRAME MATERIAL CHECK ONE, and PLASTIC box.
Determine the relevant particulars in the My signature certifies that all, Signature, HFS R, and Signature Date area.
Step 3: Select the Done button to save your file. Then it is at your disposal for transfer to your gadget.
Step 4: Create duplicates of your file. This can prevent possible challenges. We do not see or share the information you have, so be sure it is secure.
