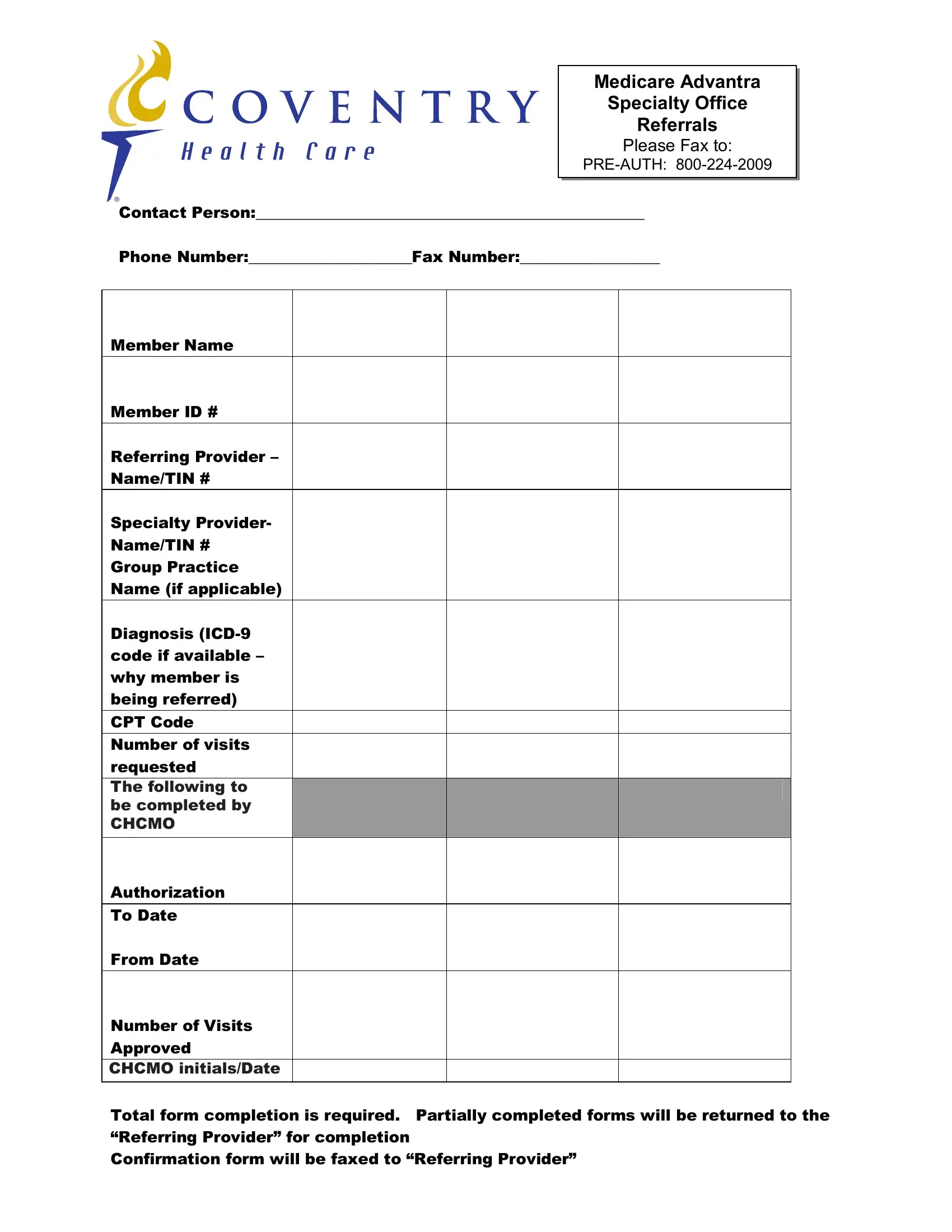
Navigating the complexities of healthcare can often feel overwhelming, especially for those under Medicare seeking specialized medical services. Key to this process is the Coventry Healthcare form, specifically designed for Medicare Advantra Specialty Office Referrals. This crucial document acts as a bridge between patients, referring providers, and specialty healthcare professionals, ensuring a seamless transition and authorization for specialized care. By submitting this form—which requires comprehensive details such as member and provider information, diagnosis codes, and the number of visits requested—healthcare providers can secure the necessary pre-authorization for their patients. This form mandates complete information to avoid delays; incomplete submissions are returned to the referring provider for completion. Additionally, a confirmation of the form's receipt and processing is reliably communicated back to the referring provider via fax. This process underscores the commitment to efficiency and communication within the healthcare system, aiming to enhance the patient experience by minimizing bureaucratic obstacles to care.
| Question | Answer |
|---|---|
| Form Name | Coventry Healthcare Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | c056957 resident health assessment form ahca 3110 1023 |
Medicare Advantra
Specialty Office
Referrals
PLEASE FAX TO:
Contact Person:__________________________________________________
Phone Number:_____________________Fax Number:__________________
Member Name
Member ID #
Referring Provider –
Name/TIN #
Specialty Provider-
Name/TIN #
Group Practice
Name (if applicable)
Diagnosis
CPT Code
Number of visits requested
The following to be
be completed by completed by GHP CHCMO
Authorization
To Date
From Date
Number of Visits
Approved
CHCMOGHP Initials/Dateinitials/Date
Total form completion is required. Partially completed forms will be returned to the “Referring Provider” for completion
Confirmation form will be faxed to “Referring Provider”