

Dealing with PDF files online is actually quite easy using our PDF tool. Anyone can fill in cw8a spanish here in a matter of minutes. Our tool is constantly evolving to give the very best user experience possible, and that is due to our resolve for continuous improvement and listening closely to customer comments. With a few easy steps, you'll be able to start your PDF journey:
Step 1: Access the form in our editor by hitting the "Get Form Button" in the top part of this webpage.
Step 2: With this advanced PDF editing tool, you could accomplish more than merely complete blanks. Edit away and make your forms appear perfect with custom textual content added, or adjust the file's original input to excellence - all comes along with an ability to incorporate stunning images and sign the file off.
This PDF doc will require you to type in specific information; to guarantee accuracy and reliability, take the time to consider the next tips:
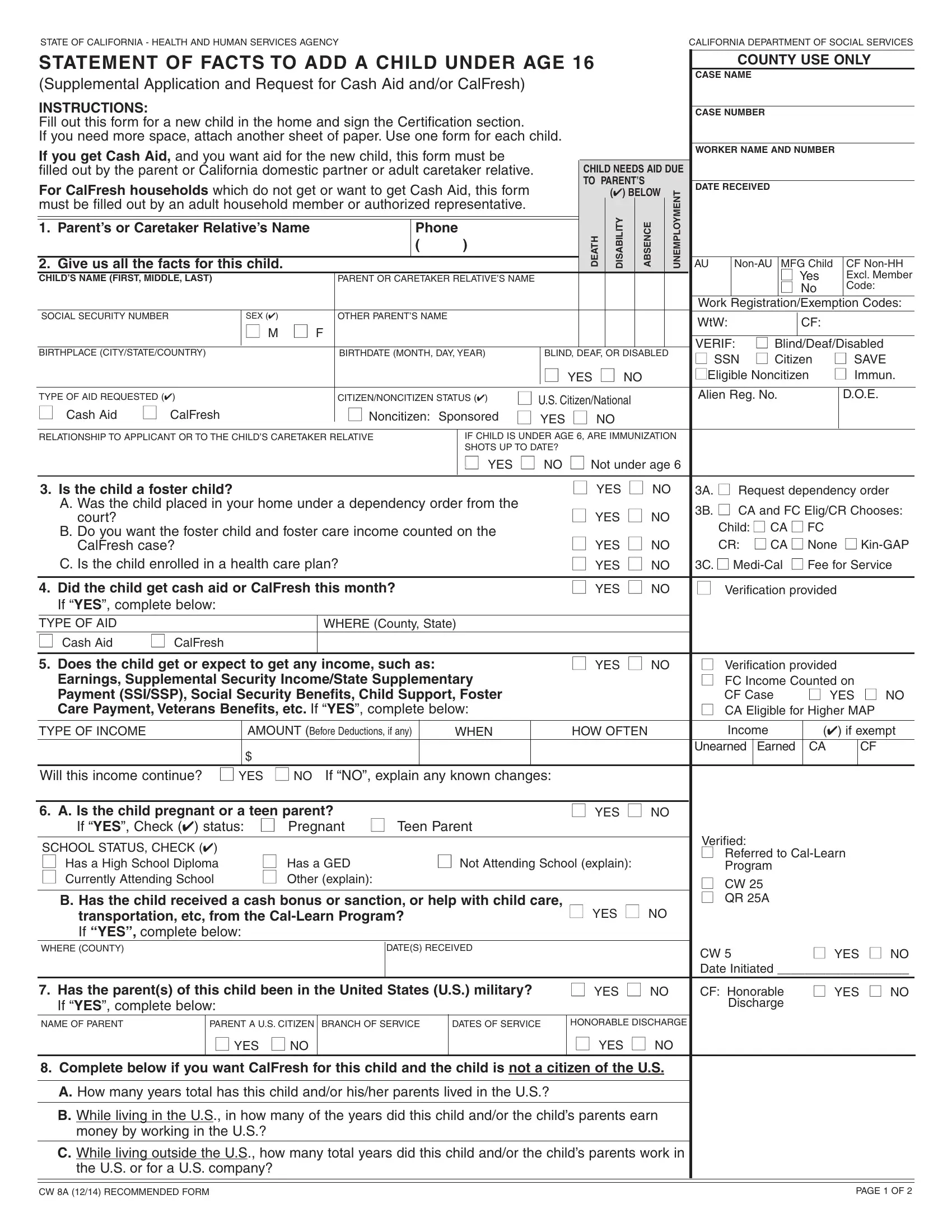
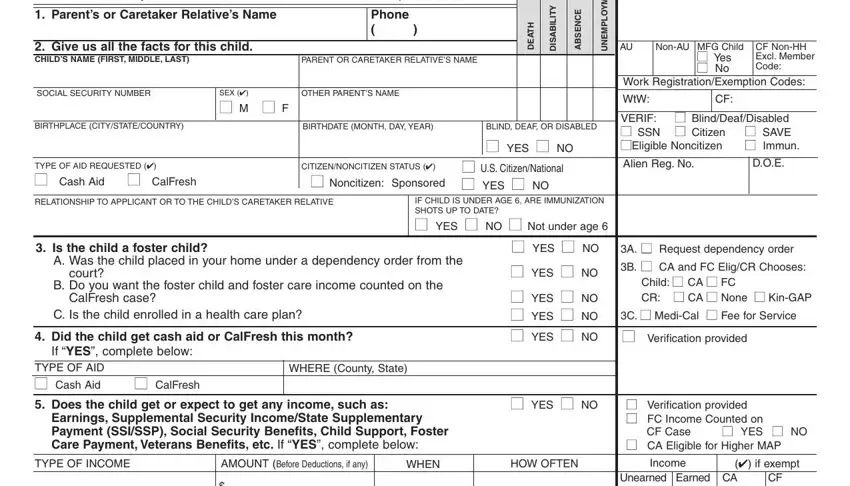
1. Begin completing the cw8a spanish with a number of essential fields. Gather all the information you need and make sure there is nothing missed!
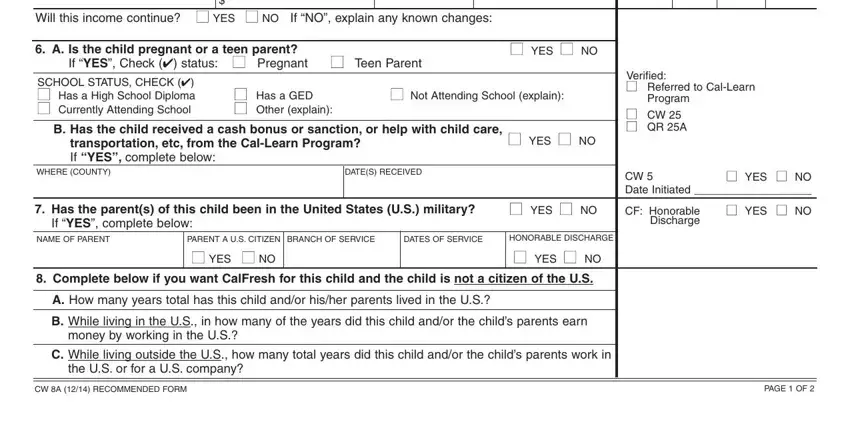
2. The next part is to submit the next few blank fields: Will this income continue YES NO, A Is the child pregnant or a teen, If YES Check status Pregnant, YES NO, SCHOOL STATUS CHECK Has a High, Has a GED Other explain, Not Attending School explain, B Has the child received a cash, transportation etc from the, WHERE COUNTY, DATES RECEIVED, YES NO, Has the parents of this child, YES NO, and If YES complete below.
3. Within this part, look at Does the child own any property, land bank accounts trust funds, TYPE OF RESOURCE, ACCOUNTPOLICY, NUMBER, NAME ADDRESS OF BANK ETC, Does the child have Medicare or, Kaiser CHAMPUS etc which is paid, YES NO, COUNTY USE ONLY, CURRENT, VALUE, YES NO, Verification provided CA, and Check if exempt CA. These should be filled in with greatest attention to detail.
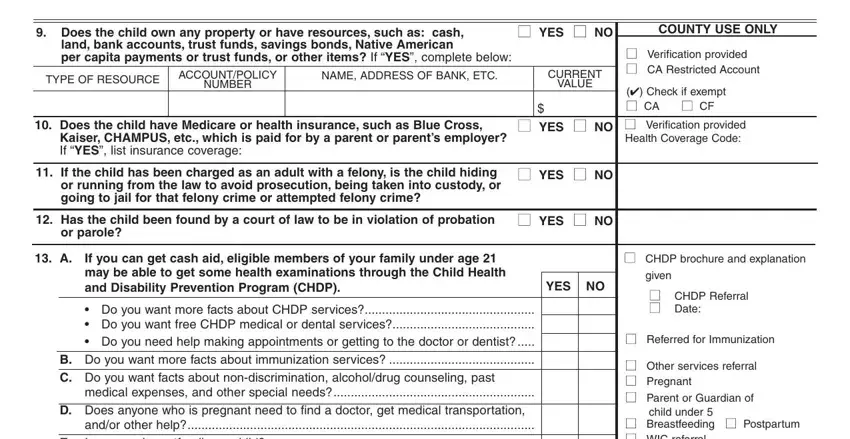
As for TYPE OF RESOURCE and Does the child have Medicare or, ensure you don't make any mistakes here. These two are certainly the key ones in the PDF.
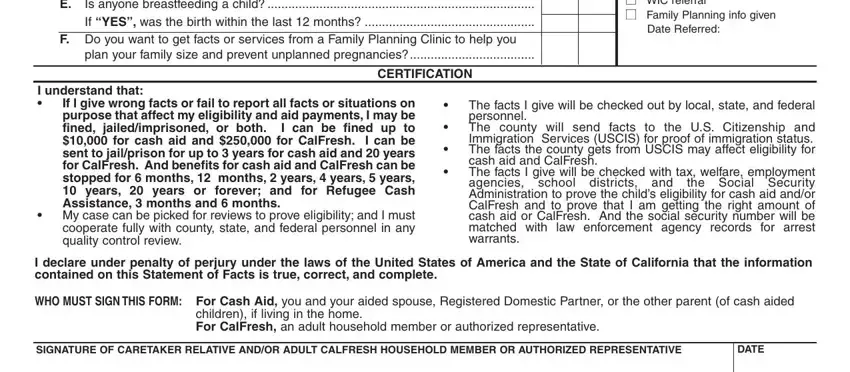
4. All set to begin working on this fourth portion! Here you will have all these andor other help Is anyone, F Do you want to get facts or, plan your family size and prevent, CERTIFICATION, Breastfeeding Postpartum WIC, Date Referred, I understand that, If I give wrong facts or fail to, My case can be picked for reviews, The facts I give will be checked, I declare under penalty of perjury, WHO MUST SIGN THIS FORM For Cash, children if living in the home For, SIGNATURE OF CARETAKER RELATIVE, and DATE blank fields to fill out.
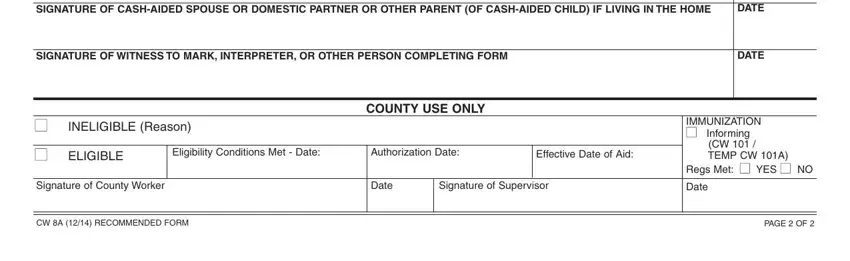
5. As you get close to the final parts of this document, there are actually a couple extra points to complete. Mainly, SIGNATURE OF CASHAIDED SPOUSE OR, DATE, SIGNATURE OF WITNESS TO MARK, DATE, INELIGIBLE Reason, COUNTY USE ONLY, ELIGIBLE, Eligibility Conditions Met Date, Authorization Date, Effective Date of Aid, IMMUNIZATION Informing, CW TEMP CW A, Regs Met YES NO, Signature of County Worker, and Date must be filled out.
Step 3: Prior to moving on, ensure that all blanks are filled in as intended. Once you determine that it is fine, click “Done." Make a free trial subscription with us and acquire immediate access to cw8a spanish - with all changes kept and accessible from your personal account. When using FormsPal, you're able to complete documents without stressing about data breaches or records getting distributed. Our protected platform ensures that your private data is maintained safely.